It’s a fast-paced world, for sure. Health care is advancing daily, and we—and our patients—continue to enjoy the fruits of researchers’ labors. Recently, investigators presented a full year’s worth of findings at the Association for Research in Vision and Ophthalmology’s (ARVO) meeting, held in Baltimore. Don’t you wish you could sit down, stop the clock and take the time to devour all the new research presented there, boosting your knowledge and clinical skills?
To give you a taste, we selected what we consider important research and reviewed abstracts for you. Hopefully they can help improve your patient care—because what’s presented today becomes practical clinical information for tomorrow. Ideas generated at this meeting spark additional research initiatives and serve to develop new strategies for diagnosing and treating a wide array of ocular disease. Take a look to see what investigators have uncovered so far:
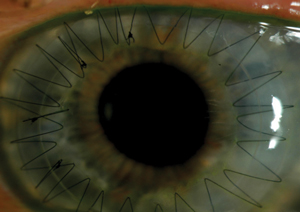 |
| Corneal transplants, such as this one, might benefit from a drug-eluting contact lens similar to the one researchers presented at ARVO. |
Corneal Infection Grand Rounds
A recent Texas-based study evaluated the efficacy of a multifaceted diagnostic approach for corneal infections. Researchers compared the results of scrape cytology and corneal cultures from the corneal washings of 47 eyes to test which diagnostic tool detected the likely cause of corneal infection best. Of the 47 cases, 14 showed culture was superior to cytology, 23 showed cytology was superior, eight showed the two to be even, one was indeterminate and one had no detection of the virus in either. The researchers concluded that culture is better for detecting bacterial organisms, while cytology is better for detecting other corneal (non-bacterial) infection causes. Accordingly, they recommend using a multifaceted diagnostic approach to ensure more accurate results since not all organisms may necessarily be detected by one method alone.1
Offering a closer look at ocular exposure to commensal organisms and their effect on immunity, a Boston study found tonic signals from local commensal flora promote ocular mucosa surveillance, in turn limiting microbial presence on the ocular surface and strengthening protection during infection. The study identified commensal species in ocular swabs from mice, then treated them with topical antibiotics to ablate bacteria in the conjunctiva. Next, the mice were rested and colonized with other commensals such as coagulase-negative Staphylococcus xylosus and Streptococcus oralis. After three weeks, the commensal strains greatly aided immunity to Pseudomonas aeruginosa. These findings show potential for commensals to regulate bacterial keratitis susceptibility.2
Another study investigated bilateral corneal endothelial cell density (ECD) and its connection to scar location and corneal nerve alterations in patients with unilateral herpes zoster ophthalmicus (HZO). Researchers compared 28 eyes with corneal scarring caused by HZO with 24 healthy eyes, using in vivo confocal microscopy (IVCM) and corneal sensation of the central cornea. Results showed significantly lower levels of ECD in scarred eyes and contralateral clinically unaffected eyes compared with healthy eyes. It also showed that location does make a difference, as central HZO scarring had notable loss of ECD compared with peripheral scars. Researchers also found a possible link between corneal innervation and corneal endothelial cell homeostasis, as results showed a positive correlation between the ECD and the subbasal nerve density in both total nerve length and corneal sensation.3
To better understand the pathophysiology of ocular infections caused by the herpes simplex virus-1 (HSV-1), researchers from the University of Illinois at Chicago explored the virus’s degradation and its supportive role for autophagy, a normal physiological process dealing with the destruction of cells.
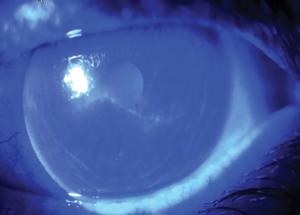 |
| Many ARVO presentations focused on Acanthamoeba keratitis, shown here with large dendriform lesion on the corneal surface. |
Autophagy maintains homeostasis by protein degradation and turnover of the destroyed cell organelles for new cell formation. During cellular stress, autophagy is increased. The study revealed that autophagy was necessary to support optimal virion growth over longer periods of time, and higher amounts of the virus were reported from cells with a normal ability to perform autophagy. In short, autophagy degrades incoming virions and then later provides support for optimal virion growth during infection. The researchers concluded that optineurin, an autophagy adapter protein of host origin, may effectively regulate the switch from virus degradation to virus support. This also marks the first substantial evidence of the dual role autophagy plays during HSV-1 infection.4
A recent study from the Yale University School of Medicine chronicled the clinical etiologies, microbial spectrum, antibiotic resistance and visual acuity outcomes of acute endophthalmitis. Tracking ICD-9 and ICD-10 codes for endophthalmitis over a six-year period revealed that the most frequent clinical etiologies were progression of corneal ulcer and postoperative infection after cataract extraction, accounting for 22% and 17% of cases, respectively.
The most likely pathogens causing endophthalmitis included coagulase-negative Staphylococcus, Staphylococcus aureus and P. aeruginosa. The vast majority of infections were deemed endogenous rather than environmental and likely relate to lid disease. Antibiotic susceptibilities were topped by vancomycin at 96.7%, closely followed by gentamicin and doxycycline, both at 96.6%. Concerning visual acuity, the majority of patients displayed improvement after treatment, but there was also a sizable portion of patients with a final visual acuity of no light perception.5
A Closer Look at Acanthamoeba keratitis
A critical amount of bacteria is required for the development of Acanthamoeba keratitis (AK), according to a new study. Researchers instilled Acanthamoeba castellanii in rabbit corneas, then instilled the organism co-incubated with high and low density P. aeruginosa. Levofloxacin eye drops were administered following each inoculation. After a five-day observation period, Acanthamoeba castellanii alone did not cause AK. Acanthamoeba castellanii co-incubated with low-density P. aeruginosa induced a few infiltrates but the cornea remained relatively clear. However, Acanthamoeba castellanii co-incubated with high-density P. aeruginosa produced severe AK. The researchers also found a six-hour co-incubation caused a much more severe case of AK than a two-hour co-incubation. The study suggests bacteria count and time of coexistence both play an essential role in AK development and severity.6
Another study found that prompt anti-amoebic treatment (AAT) and age are important factors in avoiding poor AK treatment outcomes. The researchers defined poor outcomes as having one or more of the following: corneal perforation, keratoplasty, other ocular surgery (except biopsy), 10.5 months or more of AAT and final visual acuity of 20/80 or worse attributed to AK. Those with poor treatment outcomes tended to be older, with a median age of 38 compared with 31 for those with better outcomes. Patients with poor outcomes also had longer symptom duration and more doctor visits prior to AAT. While age is simply a factor to indicate possible issues, researchers concluded that AAT intervention should begin as early as possible to give patients a better opportunity for positive AK outcomes.7
Similarly, a Philadelphia study sought to identify risk factors for AK treatment failure. Researchers tracked 60 AK patients based on demographics, clinical details, treatment protocols and overall outcomes. They defined treatment failure as requiring penetrating keratoplasty or having best-corrected visual acuity (BCVA) worse than 20/100 at the last follow up. The researchers found that 25 eyes (42%) had treatment failure; contributing factors included older age, longer duration of symptoms prior to presentation, poorer presenting BCVA and positive diagnosis on pathology. Some of the findings, however, were unexpected. Despite better disease recognition today, the researchers found worse outcomes in cases treated from 2012 to 2015 compared with cases from 2009 to 2011. In fact, the percentage of failures was much higher compared with a group treated from 2004 to 2008. Researchers recommend doctors counsel older AK patients, those with longer duration of symptoms and those with poor initial BCVA about the possibility of poor outcomes.8
 |
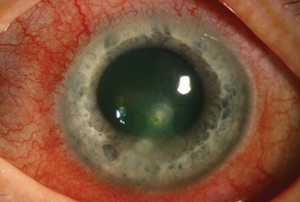
| Progressing corneal ulcers, as seen here with hypopyon, account for 22% of acute endophthalmitis, according to new research. |
At the Forefront of Dry Eye
To shed more light on the natural history of dry eye disease (DED), researchers studied 3,136 subjects—91% of whom were female—and found nearly 10% developed symptomatic DED within the two-year study timeframe. For those with symptomatic DED at baseline, up to 37% showed resolution of symptoms in two years. This closer look at the natural history of DED suggests symptomatic cases can be highly variable over time, according to researchers.
The researchers also found female sex, asthma, osteoarthritis, chronic pain syndromes, depression, higher copper intake, lower coffee intake and increased body mass index were all associated with symptomatic DED. Persistence was associated with osteoarthritis, increasing age and female sex, while resolution of symptoms was associated with stroke, use of contact lenses and higher coffee intake. A better understanding of DED’s natural history may lead to more focused clinical care, the researchers conclude.9
Using IVCM, Boston researchers have discovered patients with DED have significantly reduced nerve density in the central and peripheral corneal quadrants. Investigators took IVCM images of the central cornea and four peripheral quadrants in 46 patients with DED and 20 age- and sex-matched controls. They found the main trunk, branch and total nerve densities of the central cornea and all peripheral quadrants of patients with DED were significantly lower compared with the control group.
When comparing nerve density between the central cornea and periphery in particular, they found total nerve density was significantly higher in the central cornea than in the nasal and inferior quadrants in DED patients, while the main trunk density in the central cornea was significantly lower than in the nasal and temporal quadrants. Because DED causes ocular surface discomfort, a better understanding of corneal nerve changes may help clinicians better manage patient symptoms.10
New findings from a Boston-based study suggest that clinicians should add the evaluation of ocular pain to a comprehensive work up for dry eye patients. In a cross-sectional study of 91 patients with DED, researchers asked subjects to rate their ocular pain on a scale from one to 10 and undergo a comprehensive ophthalmic examination that included an ocular surface disease index (OSDI) questionnaire. They found 44.9% of the study subjects said they had mild pain, 33.7% indicated moderate pain and 6.8% rated their pain as severe. When the researchers assessed the patients’ pain scores in relation to their OSDI score and clinical signs, they found the ocular pain scores only correlated weakly with the OSDI scores and had no correlation at all with DED signs.11 The neuropathic features of DED continue to receive much attention, especially as it relates to resultant clinical depression.
Although previous research shows a correlation between bacterial burden and signs of meibomian gland dysfunction, a new study suggests the same is not the case for dry eye symptoms. Researchers from the Brien Holden Vision Institute asked 186 participants with normal ocular and systemic history to complete the OSDI and McMonnies dry eye questionnaires, and have a swab taken from their left lower lid margin. The results of the swab cultures and questionnaires showed only a weak correlation between dry eye symptoms and bacterial burden. The OSDI indicated 114 participants were normal, 42 had mild dry eye, 21 had moderate and eight were severe, while the McMonnies questionnaire showed 98 were normal, 76 had marginal dry eye and 12 had pathological dry eye. The swabs revealed the most common species were Propionibacterium sp. (59%) and Staphylococcus epidermidis (36%). Ultimately, the data shows no consistent trend in bacterial burden vs. the questionnaire scores.12
A new study used an online survey of ophthalmologists to gather information about DED procedures to learn more about evaluating dry eye patients for possible Sjögren’s syndrome (SS). The study found that a majority of ophthalmologists surveyed prefer to use traditional DED tests such as corneal fluorescein staining as opposed to newer tests such as tear osmolarity assessment. The survey also uncovered an abundance of under-referral of DED patients for SS work ups, which researchers suspect may be a contributing factor to underdiagnosis of SS. Some common reasons for SS referral included positive review of systems, severe dry eye symptoms or signs and dry eye resistant to treatment. The survey found 83% of respondents felt an evidence-based standardized screening tool for SS evaluation referrals in DED patients is needed.13
A new condition known as lid seal compromise may have a significant impact on refractory dry eye patients, according to a study that sought to reveal its prevalence in this patient population. Researchers used the Korb–Blackie (KB) light test to assess lid seal compromise in 46 symptomatic patients and 50 asymptomatic patients with a zero-to-three scale—zero indicated no visible lid seal compromise and three indicated severe lid seal compromise. They found 61% of symptomatic refractory dry eye patients had moderate to severe compromise compared with only 14% of the asymptomatic group. The researchers conclude lid seal compromise may be a primary deleterious factor in the etiology of dry eye, causing chronic exposure to desiccating stress during sleep.14
Another recent study looked at tear protein content following intranasal tear neurostimulation (ITN) in DED patients. The post-ITN tear samples of 55 patients were analyzed for protein concentration, using a 20% margin of the pre-stimulation mean to evaluate the equivalence between pre- and post-stimulation. The 95% confidence interval fell within the equivalence margins for mean difference in total protein concentration, relative lysozyme levels and relative lactoferrin levels. This suggests sensory neural stimulation of the nasal cavity promotes release of proteins from secretory granules in the lacrimal gland following ITN stimulation. This is critical in the lacrimal gland’s role in protection against environmental insult and the maintenance of ocular surface homeostasis, the researchers conclude.15
 |
| Research on HSV-1’s degradation and its supportive role for autophagy may one day lead to a better understanding of ocular effects of the virus, such as this central corneal ulcer and HSV stromal keratitis. |
Contact Lens Innovation
Artificial tears can impact how well pathogens adhere to conventional and silicone hydrogel contact lenses, but not all pathogens, one study found. Researchers from the University of Waterloo School of Optometry and Vision Science tested four bacterial strains—P. aeruginosa, Achromobacter xylosoxidans, Delftia acidovorans and Stenotrophomonas maltophilia—with both Acuvue 2 (etafilcon A, Johnson & Johnson Vision) and Acuvue Oasys (senofilcon A, Johnson & Johnson Vision) lenses.
In the control group, the total counts didn’t differ between the two materials, although A. xylosoxidans and P. aeruginosa were significantly higher compared with D. acidovorans. After soaking the lenses in an artificial tear solution, the senofilcon A material showed no difference in the total counts for any strain. The total counts of A. xylosoxidans and P. aeruginosa on the etafilcon A material remained significantly higher compared with D. acidovorans and S. maltophilia. In addition, the etafilcon A lenses had lower total counts of D. acidovorans compared with the senofilcon A lenses; for the remaining three strains, the total counts did not vary significantly between the two materials.16
Another study looked at pathogens on contact lenses, this time focusing on the bacterial biofilm that can grow in contact lens cases. Although disinfecting contact lens cases can remove more than 99% of the bacterial biofilm, it doesn’t necessarily keep contact lenses bacteria-free, according to researchers from the School of Optometry and Vision Science at the University of New South Wales.
After growing P. aeruginosa or S. aureus biofilms on cases, researchers added contact lenses and disinfected the cases with a multipurpose disinfecting solution or a rinsing solution for four hours. Cases following the disinfection cycle with the disinfecting solution had a significant reduction of biofilm, while the cases cleaned with the rinsing solution did not. For the cases cleaned with multipurpose solution, 26% of the remaining P. aeruginosa and 13% of remaining S. aureus were transferred to the lenses.
Although only 1% of the bacteria in the cases cleaned with rinsing solution was transferred to contact lenses, the contact lenses from storage cases disinfected with multipurpose disinfecting solution had significantly lower numbers of P. aeruginosa and S. aureus compared with lenses from storage cases filled with rinsing solution. The results emphasize the importance of properly caring for lens storage cases to prevent biofilm formation in the first place.17
Two new contact lens designs hold promise for slowing myopia progression, according to investigators at the Brien Holden Vision Institute. To test the designs—one that imposed myopic defocus across the central and peripheral retina and one that manipulated higher-order aberrations to provide retinal image quality that degraded in the direction of myopic eye growth—researchers enrolled 508 myopic children and randomized them into five groups: a control group wearing single-vision silicone hydrogel (SH) lenses, two groups wearing SH lenses with varying powers and two groups wearing hydrogel lenses. At 12 months, three of the four test groups showed significantly reduced myopia progression compared with the control group. After adjusting for age, parental myopia and compliance, they found the reduction in myopia progression with the test lenses ranged from 21% to 29% for spherical equivalents and 31% to 42% for axial length, which increased to 27% to 33% and 38% to 56%, respectively, for those who were compliant.
These results suggest both of these new designs can reduce myopia progression, the researchers conclude. This is yet another study that shows that imposing myopic defocus across both central and peripheral retina or providing retinal image quality that degrades in the direction of eye growth can provide a signal to slow eye growth.18
Clinicians can consider using wavefront-customized hydrogel contact lenses in normal eyes, as well as to modulate and correct spherical aberration and coma, according to researchers. A new study used seven customized, lathe-cut hydrogel contact lenses that incorporated specific amounts of spherical aberration and coma. When fit on three normal subjects (three eyes total), the lenses modulated the aberration in a consistent fashion towards the same polarity of the aberration, ranging from roughly 60% to more than 200% of the intended change. In addition, the lenses that employed coma of the same sign as the subject’s coma increased the coma of the eye-lens combination. Lenses with opposite coma decreased, or even reversed, the on-eye aberration coma. Custom lenses that can be personalized to each patient’s specific needs can be useful in normal eyes with subtle higher-order aberrations, the authors conclude.19
Another study evaluated a novel drug-eluting contact lens for the treatment of experimentally induced neovascularization. Using a rabbit model, researchers compared the effects of contact lenses that eluted dexamethasone with a control group treated by topical dexamethasone sodium phosphate drops hourly. They assessed corneal inflammation on day seven by analyzing CD45 cell frequencies in tissue using flow cytology. The dexamethasone-eluting contact lenses effectively inhibited corneal neovascularization and inflammation similar to the hourly-administered eye drops. Contact lens drug delivery may be an option for ocular drug delivery and the prevention of many corneal responses, including post-keratoplasty rejection episodes, the researchers conclude.20
This is just a sampling of the many wonderful research projects presented at this year’s conference. I encourage you to browse the full list to broaden your horizons beyond these select research projects. We look forward to another productive year of clinically relevant research from ARVO next year!
Dr. Shovlin is the senior optometrist at Northeastern Eye Institute and a member of the adjunct faculty at the Pennsylvania College of Optometry. He is also the clinical editor for Review of Cornea & Contact Lenses, associate clinical editor for Review of Optometry and president of the American Academy of Optometry.
1. Nakatsuka A, Ortiz J, Chevez-Barrios J. A multifaceted diagnostic approach to pathological diagnosis of corneal infection. Program 3343. Association for Research in Vision and Ophthalmology (ARVO) Meeting 2017.
2. Gadjeva M. Impact of commensals on ocular immunity to infection. Program 5772. ARVO 2017.
3. Hamrah P, Sahin A, Chirapapaisan C, et al. In vivo confocal microscopy demonstrates bilateral corneal endothelial cell loss in patients with unilateral herpes zoster ophthalmicus. Program 1483. ARVO 2017.
4. Shukla D, Thakkar N, Jaishankar D. Dual role for autophagy in herpes simplex virus infection of the cornea. Program 3619. ARVO 2017.
5. Lu L, Adelman RA. Clinical etiologies, microbial spectrum, antibiotic susceptibilities, and visual acuity outcomes of acute endophthalmitis. Program 5519. ARVO 2017.
6. Nakagawa H. Number of bacteria and time of co-incubation with bacteria required for the development of Acanthamoeba keratitis. Program 5782. ARVO 2017.
7. Carnt NA, Robaei D, Minassian D, Dart JK. Acanthamoeba keratitis in 194 patients: risk factors for poor outcomes and severe inflammatory complications. Program 4796. ARVO 2017.
8. Siu S, Rapuano CJ, Nagra P, Hammersmith K. Acanthamoeba keratitis: are recent infections more severe? Program 3891. ARVO 2017.
9. Vehof J, Hammond CJ. Incidence, persistence and resolution of dry eye disease: new insights into the natural history. Program 2700. ARVO 2017.
10. Salem Z, Gabriela Dieckmann G, Tanaka A. Patients with dry eye disease demonstrate significant decrease in central and peripheral corneal nerve density. Program 2658. ARVO 2017.
11. Sun Z , Satitpitakul V, Kheirkhah A, et al. Ocular pain in patients with dry eye disease. Program 2659. ARVO 2017.
12. Flanagan J, Yeotikar N, Zhu H, et al. Ocular bacterial burden and dry eye symptoms in a normal population. Program 2690. ARVO 2017.
13. Fernandez K, Ying GS, Masssaro-Giordano G, et al. A survey of dry eye practice patterns. Program 2651. ARVO 2017.
14. Korb DR, Blackie CA, Nau AC. Prevalence of compromised lid seal in symptomatic refractory dry eye patients and asymptomatic patients. Program 2696. ARVO 2017.
15. Woodward A, Senchyna M, Franke M, et al. Effect of intranasal neurostimulation on tear protein content in patients with dry eye. Program 2673. ARVO 2017.
16. Dantam J, Subbaraman L, Jones LW. Adhesion of emerging pathogens to contact lenses under the influence of an artificial tear solution. Program 3079. ARVO 2017.
17. Vijay AK, de Jesus NG, Ong J, Willcox MD. Bacterial transmission to contact lenses following storage case disinfection. Program 3074. ARVO 2017.
18. Sankaridurg P, Bakaraju RC, Morgan J, et al. Novel contact lenses designed to slow progress of myopia: 12 month results. Program 2391. ARVO 2017.
19. Akers D, Asimellis G, Karageorgiadis L, et al. Wavefront-customized soft contact lenses for high-order aberration correction in normal eyes. Program 1276. ARVO 2017.
20. Kobashi H, Bengani L, Ross AE, et al. Inhibition of Corneal Neovascularization by Dexamethasone-Eluting Contact Lenses in a Rabbit Model. Program 1000. ARVO 2017.

