Although contact lenses are classified as medical devices and subject to the same stringent FDA approval process as cardiac stents, orthopedic implants and any other manufactured health aid, they are increasingly seen by many as a commodity. Before the era of mass production, conventional contact lenses were lathe-cut and made to order, with varying diameters and base curves. Then, in the late 1980s, the first disposable soft contact lenses were produced using a cast-mold production process, forever changing the industry. Since then, stock lens offerings have increased exponentially. Patients enter a competitive consumer environment upon leaving the exam room, one that is complicated by a range of discount vision plans and online retailers who emphasize cost savings and little else.
Case #1: The Presbyope with Large HVID
A pair of custom center-near aspheric soft multifocals was ordered using spherical equivalent power for the distance correction. The base curve and diameter was adjusted to 8.4mm and 15.2mm OU to improve the fitting relationship. Given a pupil diameter of 4.0mm in ambient light, the center-near zone was set at 2.0mm extending to a 3.5mm intermediate zone. With these lenses, he was able to comfortably achieve 20/20 distance vision in each eye and read his phone and an iPad that he uses in the cockpit. |
In light of this downgrade of contact lenses in the public sphere—from medical device to commodity product—it is easy to see why many patients lose sight of the value of our expertise in choosing an appropriate lens. This trend is especially concerning for patients with higher demands on their vision who have struggled to find an appropriate stock lens. Educating patients regarding your ability to personalize their fit with custom-designed lenses can help you better meet their needs and stand apart from competition.
Potential Candidates
By definition, a custom contact lens is any soft, gas permeable (GP) or hybrid lens design that is made to order, with multiple design parameters that can be manipulated. Although irregular cornea applications may come to mind first as the best use of custom lenses, they can address many patients' refractive needs that are not being met with standard “off-the-rack” disposable contact lenses.
• Astigmatic Patients. How often do patients mention they have been told they cannot wear contact lenses because of their astigmatism? An estimated 90% of astigmatic patients can be fit in the parameters available with stock soft toric lenses, which typically includes a range of +6.00D to -9.00D in spherical power and up to -2.25D cylinder power.1 For patients outside of this range, custom soft toric lenses are an option. Depending on the laboratory, from 8.00D up to 12.00D of astigmatism can be incorporated with one-degree axis steps. With larger amounts of astigmatism, cylindrical axis refinement is critical. Custom lenses can be lathe-cut to nearly any base curve, diameter and prism to improve rotational stability.
| Case #2: The High Astigmat A 24-year-old graduate student presented wearing soft toric lenses, but only part-time because he reported that vision is better in spectacles. In addition to better clarity when using spectacles, he reported fluctuating vision when blinking in his contact lenses.
Custom soft toric lenses were empirically ordered using the Definitive (efrofilcon A, Contamac) material. Given his significant level of myopia and thicker lens periphery, a silicone hydrogel material was preferable. After vertexing, the following lenses were ordered: -9.25 2.75x005 with an 8.2 base curve and 14.8 diameter OD and -10.25 1.75x160 with an 8.3mm base curve and 14.8mm diameter. He was able to achieve stable, 20/20 vision in each eye and was thrilled with his vision. He is now wearing his contact lenses daily. |
When patients express a desire for better vision, consider discussing GP lenses, as they offer a superior quality of vision compared with soft toric lenses.2,3 As a general rule of thumb, spherical GPs can be used when refractive astigmatism equals corneal astigmatism of less than 2.5D. If there is any residual astigmatism, it can be applied to the front surface. However, in cases of higher corneal astigmatism, back-surface or bi-toric GPs are typically used.
If initial comfort with corneal GP lenses is a concern, consider prescribing hybrid or scleral lenses instead. Many GP laboratories are now marketing smaller diameter scleral lenses to fit the “normal” cornea. These specialty lenses provide stable, higher quality vision with comfort rivaling soft toric lenses.4
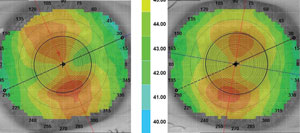
• Corneal Shape. Most stock soft lenses take a “one-size-fits-all” approach, with only one diameter and one base curve to choose from. If two base curves are available, however, the choice is most often made using keratometry readings. Sagittal depth of the cornea, which is influenced by corneal diameter, may also play a significant role in the lens-cornea fitting relationship. Corneal diameter is typically measured by horizontal visible iris diameter (HVID), with average corneal diameter measuring 11.8mm.5,6 Patients with an HVID outside the typical range can expect a lens to decenter, reducing both the patient’s quality of vision and comfort. To solve this, base curves and diameter can be manipulated with custom lenses to change the overall sagittal depth of a lens and thus better match corneal shape.
• Presbyopes. The strain placed on near vision in our technology-driven world, coupled with the influx of presbyopic patients, has put multifocal lenses more in demand than ever. The ability to change multiple design parameters once again increases the odds for success. Knowing the patient’s desired working distance can help in the decision-making process. If higher add powers are required, many GP multifocals have adds greater than 3.0D. Certain custom laboratories such as SpecialEyes can manufacture lenses with an add power up to 4.0D at 0.10D increments.
A 23-year-old professional baseball player presented to the office for contact lens evaluation. He was wearing standard soft toric lenses, but complained of fluctuating vision. As a competitive athlete, it was critical that his vision be as crisp and stable as possible. His Rx was +1.00 1.75x097 OD +1.25 2.00x071 OS, with keratometry readings of 41.75/43.00 at 003 OD and 41.75/43.50 at 167 OS. We selected hybrid lenses to provide GP optics without the concern for lens rotation or dislodgement. The lenses provided 20/15 vision in each eye. The patient reported they were both comfortable. |
Most gas permeable and custom soft multifocals rely on aspheric, simultaneous vision designs. Depending on the specific design of the lens, adjusting zone sizes inf relation to pupil size can improve the optics. For example, if a center-distance, aspheric GP multifocal has a standard distance zone of 3.95mm, patients with a smaller pupil diameter may have difficulty achieving great near vision, while those with larger pupil diameters may have shadowing and glare at distance, especially in scotopic conditions. Center-near custom soft multifocals allow both near and intermediate peripheral zones to be adjusted dependent on pupil size.
Patients looking for crisp, uninterrupted vision at both distance and near may do better in a translating GP multifocal because it avoids the inherent limitations of simultaneous vision designs. However, pay careful attention to lower lid anatomy before beginning the fitting process to make sure the lens can rest appropriately on the lid and translate upward as needed. The lower lid should be at or within 1mm from the limbus, without significant laxity, to allow for appropriate translation. If centration or comfort is a concern, you may consider fitting hybrid or scleral multifocals. Scleral multifocals may serve a dual purpose—that is, correcting presbyopic refractive error and treating underlying dry eye.
• Myopia Control. Many practitioners are now using contact lenses for myopia control—in fact, an audience poll at the 2014 American Optometric Association (AOA) annual meeting found that 32% of participants prescribed soft multifocal lenses and 29% prescribed orthokeratology lenses for this purpose.7
A recent myopia control study with soft multifocal contact lenses used a center-distance design with a +2.00D to reduce peripheral blur.8 Currently, the only mass-produced lenses that can provide such a design include the Biofinity Multifocal (Cooper Vision), Proclear Multifocal (Cooper Vision) and Acuvue Oasys for Presbyopia (Johnson & Johnson Vision Care). This presents an opportunity for a custom multifocal. The ability to adjust zone sizes, incorporate astigmatism power and increase the add power, if tolerated, can increase the likelihood of successful wear. Additionally, a custom lens may help reinforce both the off-label nature and extra level of care you are providing to the patient.
Orthokeratology lenses, which are custom GPs with a reverse geometry design, for corneal correction if daytime lens wear is either uncomfortable or not an option due to environmental or occupational reasons. These lenses are more commonly prescribed for children, but can be worn by adults as well and are fit both diagnostically and empirically.
Personalized Fitting
Identifying candidates for custom contact lenses begins with taking a case history. Many non-contact lens wearers believe their prescriptions exclude them from contact lens wear. Similarly, for both current and former contact lens patients, inquiring about their wearing experiences can help you better tailor a custom lens option for them. Once the need for a custom lens is established, patients can be fit diagnostically or empirically.
Diagnostic fitting evaluates the lens-to-cornea fitting relationship of various lenses; however, this approach may increase chair time during the initial evaluation. Certain lenses, including translating GPs and scleral lenses, are better fit diagnostically.
Because most practices do not carry a large GP inventory or multiple diagnostic sets, empirically ordering GP lenses is often the preferred approach for many practitioners. In addition to potentially reducing chair time, empirically designed GPs have been proven to be accurate.4 When ordering empirically, manifest refraction and keratometry readings are required for GP, hybrid and custom soft lenses. Choosing the initial lens diameter for a GP lens can be done after assessing the upper eyelid position. Generally, if the eyelid is positioned at or near the upper limbus, a lid-attached fit can be achieved with a diameter of 9.4mm or greater. An interpalpebral fit may require a smaller, steeper lens with a diameter of 9.2mm or less.
Fitting toric GPs may seem intimidating, but there are multiple fitting nomograms and resources available to help design these lenses, such as www.gpli.info/lens-calculator/. Using spectacle refraction and keratometric readings, the lens calculator will recommend either a spherical or toric GP lens, and will provide parameters. For presbyopic patients being fit with either GP or custom soft multifocals, measuring pupil size in both photopic and scotopic conditions can help determine initial zone sizes. Keep in mind that add power may vary depending on the patients’ most desired working distance.
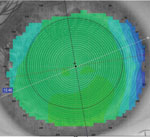
Corneal topography is a great tool to use when fitting custom lenses. Multiple measurements such as keratometric readings, HVID, pupil size and corneal eccentricity can be obtained in a matter of minutes. Additionally, many topography software programs can simulate sodium fluorescein patterns of a calculated contact lens.
Custom lenses also differ in care requirements compared to “off-the-rack” lenses. Replacement schedules vary depending on the type of lens and the discretion of the prescribing doctor, but typically range from quarterly to annually. Proper care and disinfection is essential to maintaining the life of each lens. In addition to standard disinfection systems, additional solvent cleaners or enzymatic cleaners can be used periodically.
Custom contact lenses can be a tough sell to patients used to the simplicity of online ordering and instant gratification. But just as a tailored suit looks and feels better than a department store’s in-stock options, lenses created expressly for each individual’s visual needs and ocular anatomy will perform better. With a little extra attention during the fit and careful patient education, you can create a truly individualized approach that gives patients superior outcomes and reinforces your expertise. The result? Happier, more loyal patients and a healthier bottom line.
Dr. Ensley is in private practice in Louisville, Ky., where he specializes in fitting specialty contact lenses. He completed a residency in cornea and contact lenses at the University of Missouri-Saint Louis and is a Fellow of the American Academy of Optometry.
1. Young G, Sulley A, Hunt C. Prevalence of astigmatism in relation to soft contact lens fitting. Eye & Contact Lens. 2011;37(1):20-5.2. Michaud L, Barriault C, Dionne A, Karwatsky P. Empirical fitting of soft or rigid gas-permeable contact lenses for the correction of moderate to severe refractive astigmatism: A comparative study. Optometry. 2009 Jul;80:375-83.
3. Fonn D, Gauthier CA, Pritchard N. Patient preferences and comparative ocular responses to rigid and soft contact lenses. Optom Vis Sci.1995;72(12):857-63.
4. Michaud L, Woo S, Dinardo A, et al. Clinical evaluation of a large diameter rigid gas-permeable lens for the correction of refractive astigmatism. Poster presented at the American Academy of Optometry Annual Meeting. 2012; Phoenix, AZ.
5. Douthwaite WA. Initial selection of soft contact lenses based on corneal characteristics. CLAO J. 2002. Oct;28:202-5.
6. Caroline P, André M. The effect of corneal diameter on soft lens fitting, part 1. Contact Lens Spectrum. 2002;17(4)56.
7. Quinn TG, Walline JJ, Sonsino J, et al. Controversies in contact lens care. Contact Lens Spectrum. 2015;30(1):34-40.8. Walline JJ, Greiner KL, McVey ME, Jones-Jordan LA. Mulitfocal contact lens myopia control. Optom Vis Sci. 2013;90:07-1214.

