Most eye care practitioners are familiar with topographical central islands caused by excimer laser refractive surgery. Observed mostly in the 1990s, this complication of PRK and LASIK is caused by the plume of evaporated stromal tissue impeding central ablation by a broadband excimer laser. The resulting corneal irregularity reduces best spectacle-corrected visual acuity. The advance of multi-zone, multi-pass excimer ablation, however, has led to a reduction of these so-called central islands.
Perhaps less recognized, overnight corneal reshaping using contact lenses (i.e., orthokeratology) can sometimes create central islands. Characteristics of patients predisposed to develop central islands in this manner are unknown. Discontinuing corneal reshaping would resolve them, but also contradict the patient’s desire to undergo corneal reshaping. Hence, it is preferable to continue with corneal reshaping while looking for other means to handle central island development.
|
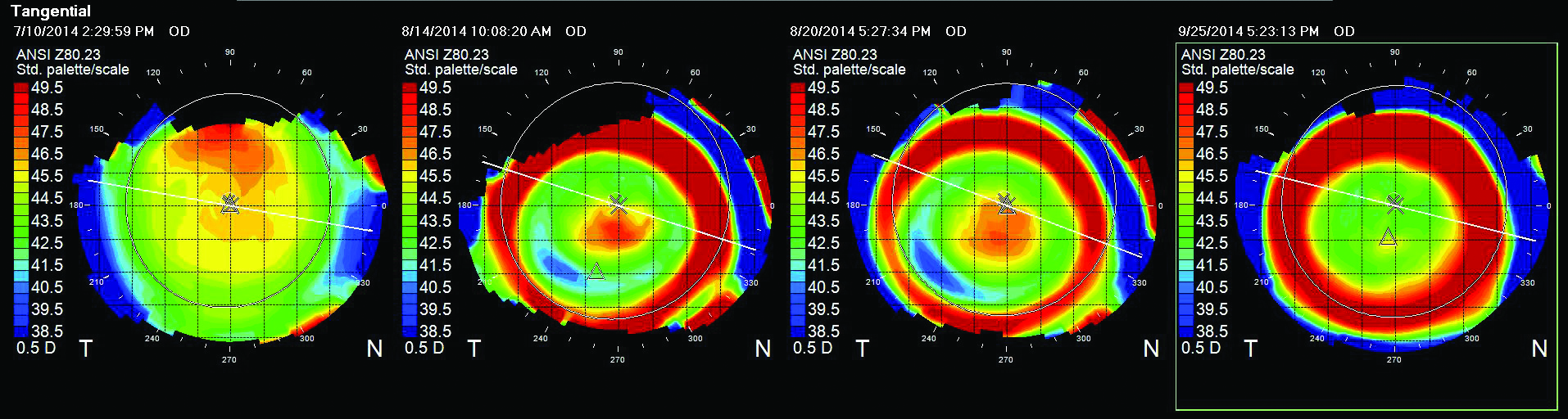
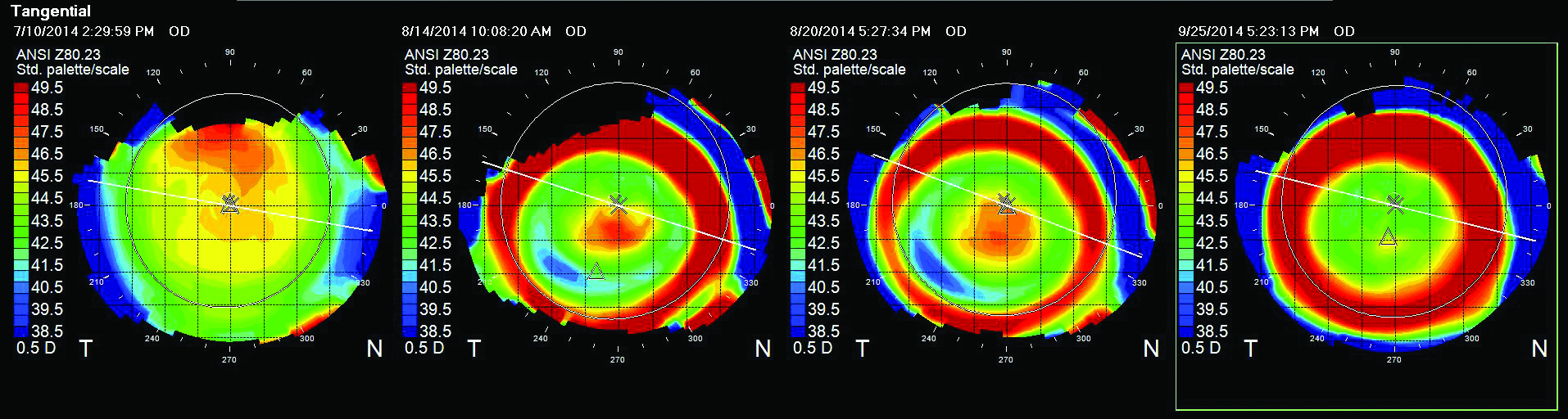
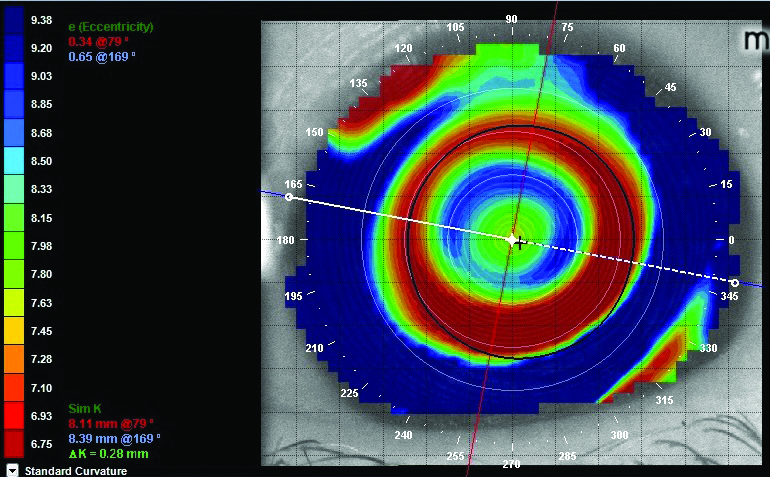
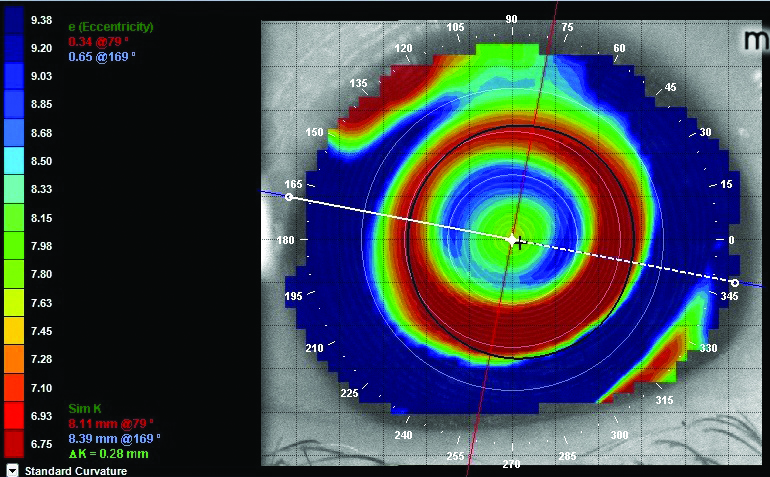
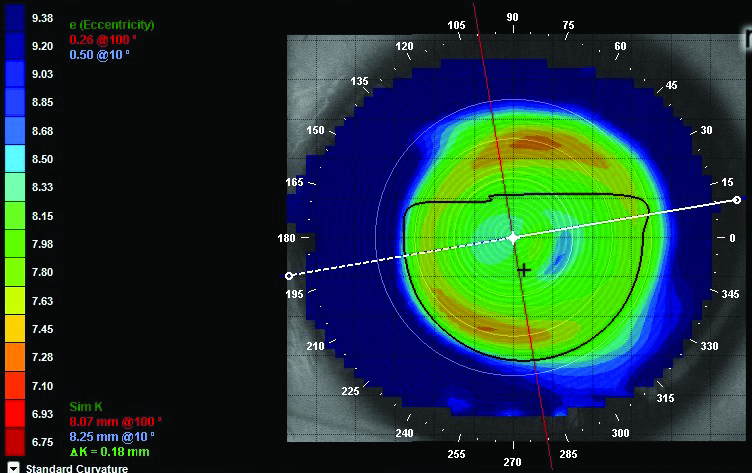
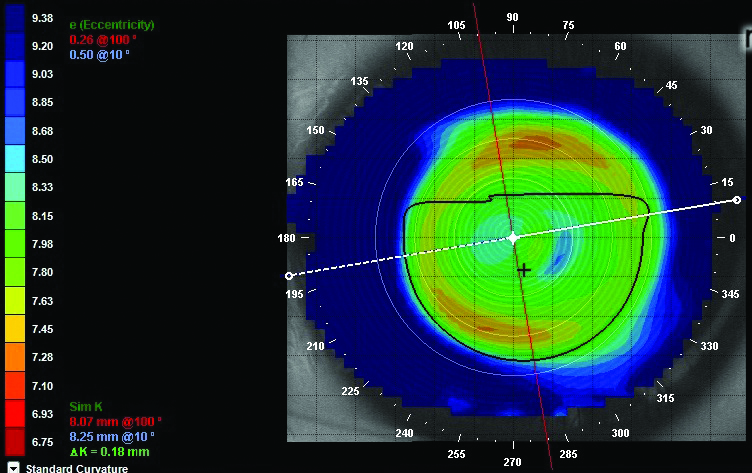
| Fig. 1. Right eye trend analysis of tangential topographies. From left to right: (a) pre-treatment; (b) one week after initiating CRT showing central island; (c) six days after CRT with RZD decreased by 25µm; and (d) three weeks after CRT with RZD increased by 25µm from the original lens. |
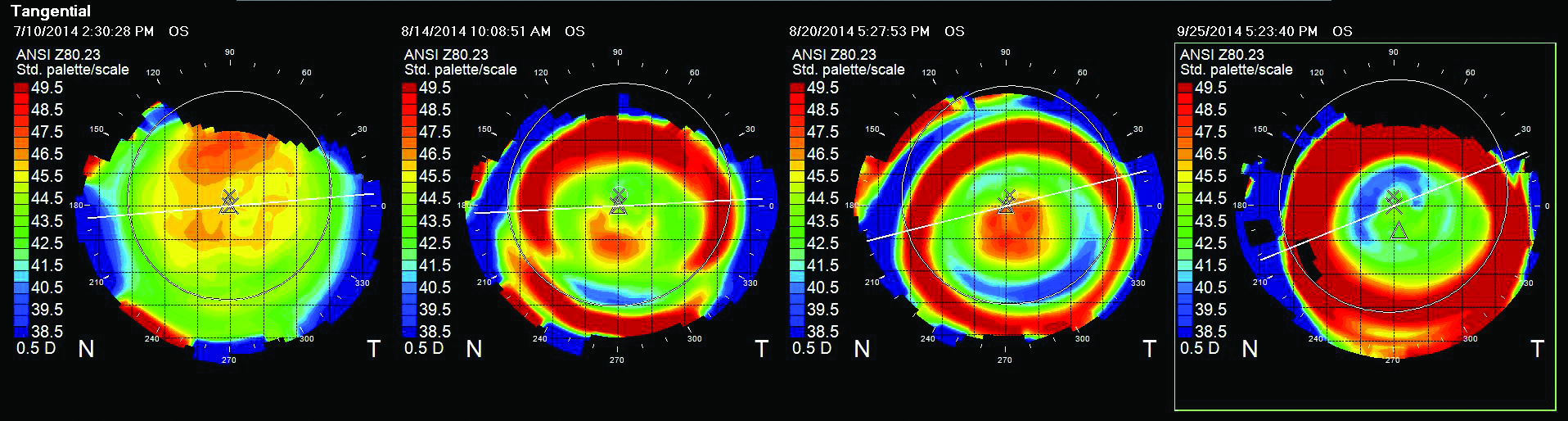 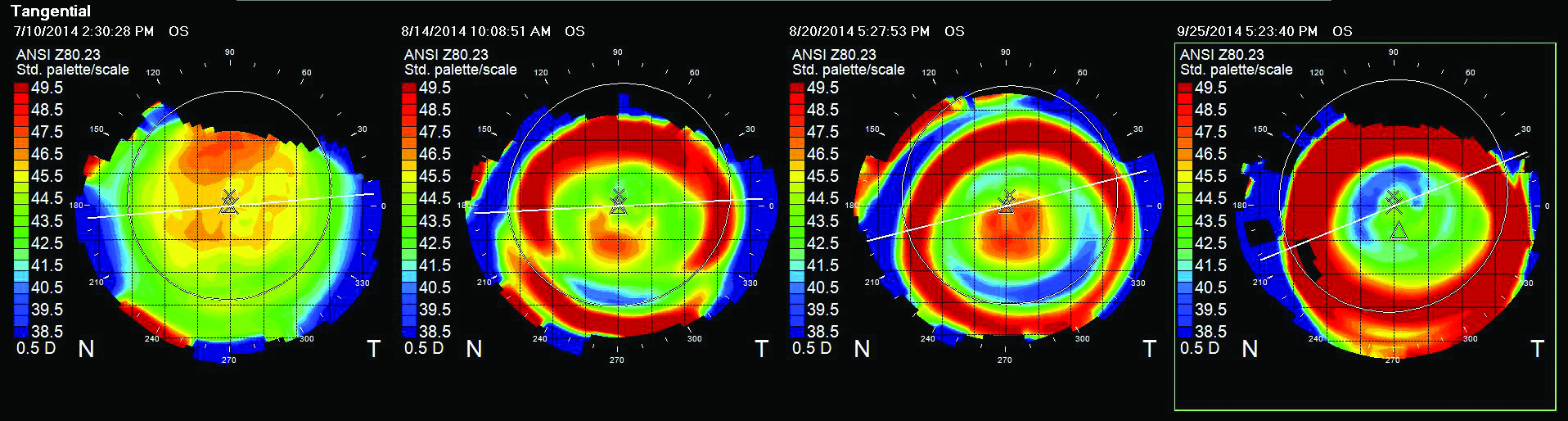 |
| Fig. 2. Left eye trend analysis of tangential topographies. From left to right: (a) pre-treatment; (b) one week after initiating CRT showing central island; (c) six days after CRT with RZD decreased by 25µm; and (d) three weeks after CRT with RZD increased by 50µm from the original lens. |
Central islands in corneal reshaping are generally accepted to result from excessive sagittal depth.1-4 With the particular implementation of ortho-K known as corneal refractive therapy (CRT, Paragon Vision Sciences), sagittal depth is most easily decreased by reducing return zone depth (RZD). It is usually recommended that practitioners reduce RZD by 25µm while maintaining all other parameters (base curve and landing zone angle or LZA).1 Reducing RZD, however, can cause lens instability, induced astigmatism and myopic regression, and also does not guarantee elimination of central islands. In fact, this case demonstrates how reducing RZD worsened central islands and how their resolution actually required increasing RZD.
Case Report
An 11-year-old Asian female underwent corneal refractive therapy. Her pre-CRT ocular health status was unremarkable and non-contributory at all visits. UCVA was OD 20/200, OS 20/200. Manifest refraction was OD -3.50-0.50X075 (20/20+) and OS -3.75-0.50X125 (20/20+). Topographies were prolate and unremarkable (Figures 1a and 2a). CRT lenses were dispensed OU according to the Paragon’s CRT lens selection nomogram, with 8.2 BC / 550 RZD / 34 LZA in each eye. One week later, UCVA had improved to OD 20/80 and OS 20/40, with manifest refraction OD pl-1.75X070 (20/40) and OS -0.75-1.00X090 (20/25+). Topography showed central islands OU (Figures 1b and 2b).
Per the manufacturer’s guidelines, RZD was decreased by 25µm OU and she began wearing 8.3 BC / 525 RZD / 34 LZA, which still provided reasonable centration and lens stability. Six days later, UCVA was OD 20/80 OD and OS, with manifest refraction OD -3.50-0.75X050 (20/25) and OS -6.00DS (20/25). On topography, the central islands were more pronounced in each eye (Figures 1c and 2c).
New CRT lenses were dispensed with OD 8.3 BC / 575 RZD / 34 LZA and OS 8.4 BC / 600 RZD / 34 LZA. Three weeks later, UCVA was OD 20/20- and OS 20/30, with manifest refraction OD -0.50-0.50X075 (20/15-) and OS -0.75-0.50X130 (20/25). Topography showed the central islands resolved in the right eye almost completely and in the left eye partially (Figures 1d and 2d).
Opposites Attract
This case illustrates how the typical procedure of decreasing RZD for central islands can sometimes make them more pronounced. For this patient, increasing sagittal depth resolved the central island in the right eye and partially resolved it in the left eye.
Kopp et al. observed that decreasing LZA by one degree leads to enough of a sagittal depth decrease (approximately 15µm) to allow the entire lens to settle closer to the corneal surface and “squash” most central islands. The LZA change does not significantly affect lens centration. The group also found that decreasing sagittal depth by decreasing RZD did not eliminate central islands. Instead, increasing sagittal depth via an RZD increase typically eliminated the central island, as it did in this case report.
  | |
| Fig. 3. A well-centered treatment zone with a central island indicates a sag reduction (LZA decrease) to “squash” the raised central area. | |
  | |
| Fig. 4. Decentered treatment zone with a central island indicates a deeper sag (RZD) is needed to create the necessary pressure in all meridians to show the completed circle of raised epithelium. |
According to Kopp, the post-treatment tangential topographic map should guide the strategy for resolving central islands. Usually, if the tangential map shows a well-centered treatment zone with a full circle of mid-peripheral steepening but with a central island (Figure 3), decreasing LZA effectively eliminates the central island.
However, as Kopp found, if the tangential map shows an incomplete ring of mid-peripheral steepening in addition to a central island (Figure 4), increasing the RZD by 25µm could resolve the central island. You can see in this topography there is not enough reshaping in the horizontal meridian to match the mid-peripheral steepening in the vertical meridian. Increasing the RZD 25µm allows more pressure in the periphery (in all meridians at an 8mm chord) to fill in the epithelial ring and complete the “closed system” necessary for an appropriate tear volume for complete myopic treatment. In this example, the central island would be minimized with a new lens with increased sagittal depth. Oval (vs. round) treatment zones also suggest inadequate sagittal depth and a need for the practitioner to increase RZD.
In summary, this case suggests central islands may be treated by decreasing LZA by one degree while keeping other parameters the same. Alternatively, when peripheral steepening does not form a complete circle on tangential topography, RZD may be increased by 25µm while keeping other parameters the same.
It is important to note this case may not reflect recommendations for central islands induced from wearing ortho-K lens designs that differ from the CRT approach. Also, more research with a larger patient sample size is welcome.
The authors wish to thank Ken Kopp, FCLSA, at Paragon Vision Sciences for his assistance with this report.
Drs. Chou and Michel practice at EyeLux Optometry, one of the largest contact lens practices in San Diego.
1. Paragon Vision Sciences. Professional Fitting and Information Guide for Paragon CRT or Paragon CRT 100. Available at: https://artoptical.com/files/documents/resources/ParagonCRTFittingGuide04-04.pdf. Accessed October 17, 2014.
2. Jackson J. Central Island Topography Patterns and Increase in Myopia with Overnight Corneal Refractive Therapy. Poster presented at the Annual American Academy of Optometry Meeting, 2002.
3. Taub, MB. Corneal refractive therapy (CRT): An alternative method of vision correction. Optometry Today, Available at www.optometry.co.uk/uploads/articles/b09d18b658e5003ce67fe8084adf1eae_taub20030516.pdf. Accessed October 17, 2014
4. McCampbell K, Bennett ES, Rah MJ. Corneal Reshaping Made Easy. Contact Lens Spectrum. October 2014. Available at www.clspectrum.com/articleviewer.aspx?articleID=12676

