 |
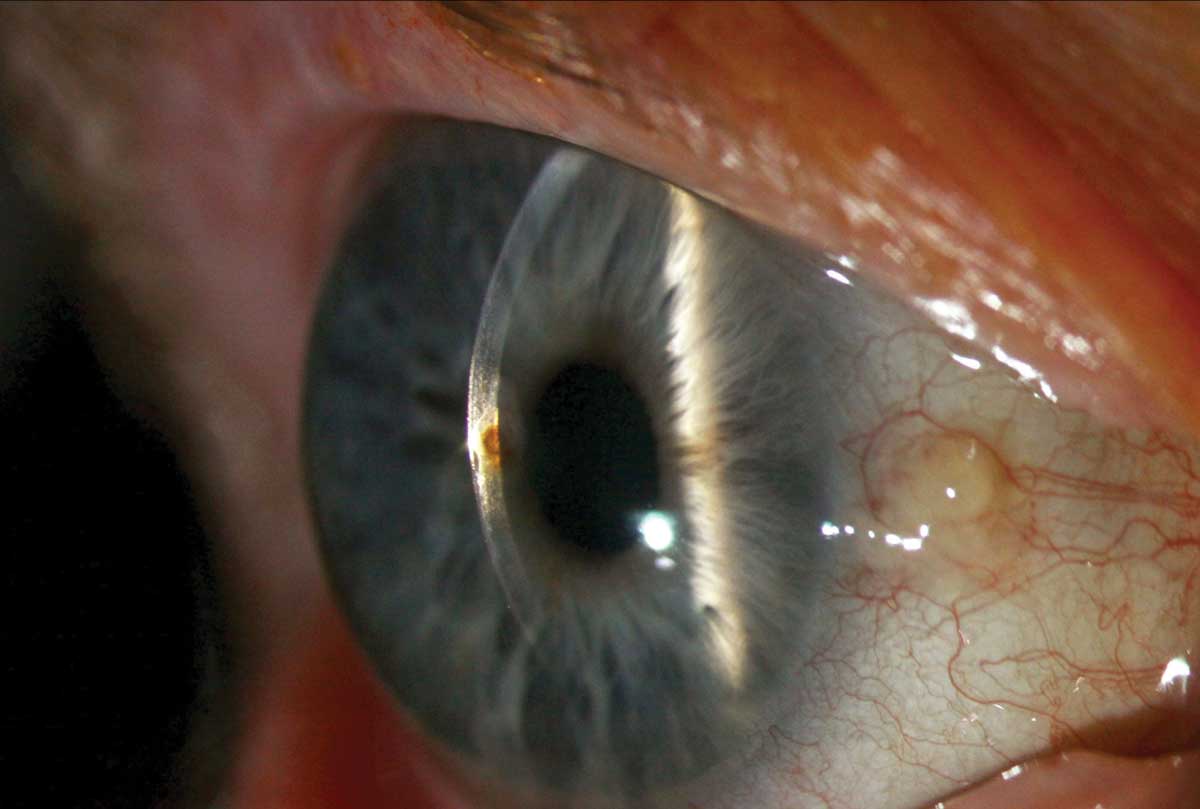
A 38-year-old male presented complaining of foreign body sensation OD. One day earlier, he had been working on some equipment when he thought something flew into his eye. He rinsed his eye with contact lens solution, and the sensation improved. However, he woke up the next morning with a gritty feeling and photophobia. His vision was slightly diminished at 20/20-2. Examination showed a single central rust ring with an overlying epithelial defect. Corneal infiltrates circumscribed the rust ring. The wound was Seidel negative. The pupil was round and reactive, and the anterior chamber was quiet.
 |
|
Photos by Sarah Skiles, ophthalmic photographer, University of Iowa. Click image to enlarge. |
Most of the rust was removed using a golf club spud, taking care not to penetrate too deeply into the stroma. Cycloplegia and a bandage lens improved comfort. The patient was put on moxifloxacin 0.5% QID and instructed to return the next day.
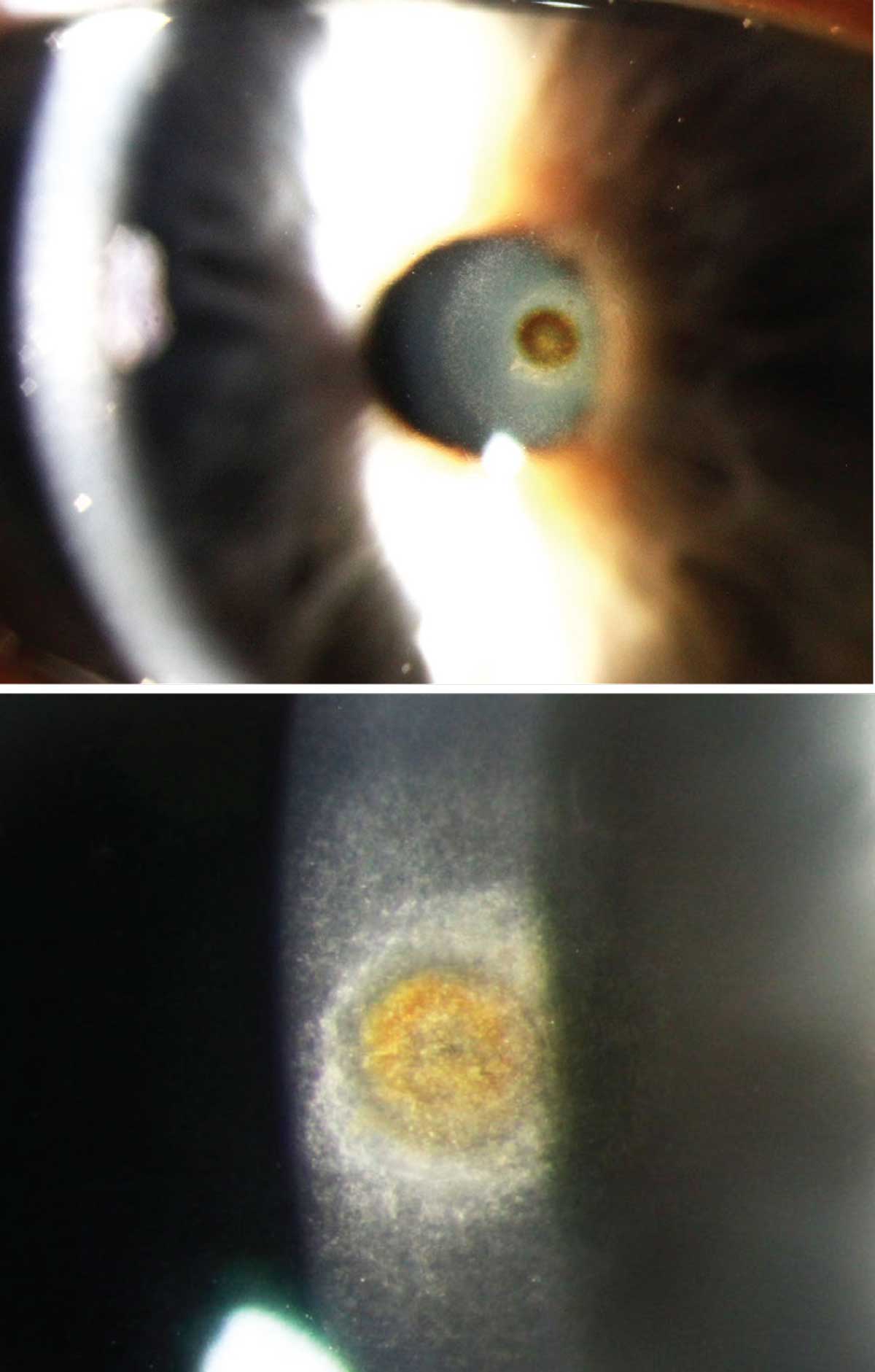
Rust rings are created when an iron-containing foreign body lodges in the corneal surface and oxidizes from salt in the tears. Formation typically starts at the level of the
 |
| Click image to enlarge. |
superficial stroma within a few hours. White blood cells (WBCs) drawn to the damaged tissue secrete collagenase, which causes the adjacent collagen to soften and break down.
The presence of WBCs indicates an inflammatory response to tissue damage and not necessarily an infectious process. It is hypothesized that soluble iron complexes react with the softened collagen to create the classic bull’s-eye rust ring. This progressive damage may be why it is often easier to remove a rust ring two to three days after the injury.
A small rust ring may be of no consequence and heal regardless of removal. However, it is standard of care to remove any remaining foreign material and as much of the rust as possible when there is visible necrosis. Rust may be removed with a cotton-tipped applicator, small-gauge needle, golf club spud, magnetic spud or Alger brush. Use caution to avoid drilling too deep or creating a bigger wound. If residual rust remains, it should be monitored and removed later if it is impeding the healing process.
Our patient returned the next day with a nearly closed epithelium, minimal residual rust and only mild foreign body sensation. Residual scarring was discussed with the patient, but his vision remained acceptable at 20/20-2. Safety goggles were advised to avoid future events.

