 |
A 49-year-old male was referred for an evaluation of a corneal problem he had in his right eye. He had been seen recently for a routine evaluation by his primary OD who thought he should make an appointment at a cornea clinic. The patient had no concerns with his vision or comfort and was simply following up on his doctor’s orders.
Preliminary Testing
Entrance testing showed spectacle corrected vision of 20/20 OU. The patient had a full range of motility with extraocular muscle function, a full confrontation field, normal pupils and intraocular pressures of 14mm Hg OD and 15mm Hg OS.
The slit lamp exam of the patient’s left eye was normal. His right eye was normal with the exception of the cornea, which was remarkable. The patient had a grayish feathery zone of anterior corneal tissue, which progressed from his 4 o’clock limbus to just below his visual axis in a whorled pattern. A thin optic section localized the irregularity in the epithelial layer. On close scrutinization, the lesion appeared to be a confluence of microcystic changes. The lesion did not stain positively or negatively with sodium fluorescein.
Corneal topography showed a small area of steepening near the corneal irregularity, though it was mild and outside of the visual axis, and a negative posterior elevation close to the lesion. Interestingly, even though the lesion was in the far anterior cornea, there was no corresponding zone of anterior elevation abnormality.
The Problem
My assessment was Lisch corneal dystrophy in the right eye on the basis of clinical evaluation alone. I asked the patient about his family history, which was unremarkable. As he was asymptomatic, I did not offer him treatment and asked him to follow up in six months.
Lisch corneal dystrophy, sometimes referred to as band-shaped, whorled microcystic corneal dystrophy, is a relatively recently recognized corneal dystrophy, having first been described in 1992, and is currently recognized in the epithelial/subepithelial group by the International Classification of Corneal Dystrophies.1,2 It is characterized as a unilateral or bilateral condition that affects the corneal epithelial tissue sectorally.
The lesions are gray and feathery in appearance and frequently present in a whorled pattern. Upon high magnification slit lamp examination, the lesions appear to be clusters of microcystic epithelial tissue. These cystic changes are most prominent on retroillumination. Given the whorled pattern sweeping from the limbus centrally, the condition looks somewhat like limbal stem cell dysfunction or advancing wavelike epitheliopathy. The involved epithelium in these other pathologies, however, tends to be coarse and gray rather than cystic.
On histology, light microscopy of the involved epithelium shows remarkable vacuolization of the cytoplasm of the cells, which are mostly optically empty.3 Pedigree analysis suggests the dystrophy is inherited in an X-linked dominant fashion.
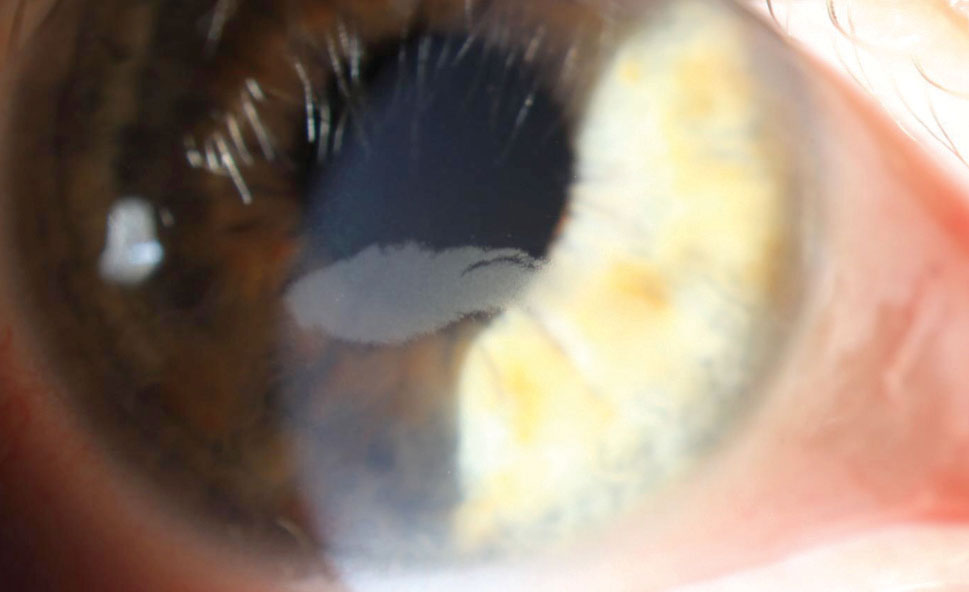 |
| The lesion is connected to the 4 o’clock limbus. Note the cystic appearance, which is most obvious at the margins. |
Though there has been debate on whether it represents a truly unique corneal dystrophy and is not just a limited subtype of Meesmann microcystic corneal dystrophy, genetic analysis demonstrates abnormalities in different chromosomes of each dystrophy, indicating they are separate entities.4
Reduction of acuity predictably results when the visual axis is involved. Though mild topographic changes may accompany Lisch corneal dystrophy, its effects on vision are driven more by the ensuing opacification of the cornea rather than the induction of irregular astigmatism. Unlike the other anterior corneal dystrophies (most notably, epithelial basement membrane and Meesmann), patients with Lisch do not develop corneal erosions.4
Solutions
Best practices for the treatment of Lisch dystrophy have not been established. Obviously, asymptomatic patients don’t need intervention beyond observation. For patients who are bothered by their vision, daily contact lens use may induce some degree of lesion regression, though this is temporary with the lesion returning on cessation of lens wear. This phenomenon has also been reported in patients with Meesmann corneal dystrophy or Fabry disease. Transient contact lens-induced epithelial thinning and hypoxia ruse may be responsible.5
For those with more severe pathology, debridement is effective in eliminating the dystrophic epithelium. This debridement may be paired with mitomycin-C (MMC) application; however, recurrence has been shown to occur frequently with or without MMC use. Recognizing that the whorled appearance and tendency for the dystrophy to recur in the same zone following debridement suggests limbal involvement. Researchers paired debridement with focal limbal cautery of the involved limbus in an eye with Lisch dystrophy that had recurred twice with debridement alone. This treatment resulted in clearance of the dystrophy, with no subsequent recurrence over two years, though its application should be limited to small areas of the limbus given the ramifications of damaging large zones of limbal tissue.6
Lisch corneal dystrophy is a newly described entity and may not be too familiar to many of us in practice. Indeed, in my practice, despite over 60 years of cumulative experience, neither corneal specialist I work with nor my colleague or I had seen a case of Lisch dystrophy in our careers prior to this patient.
Interestingly, in the last 18 months alone, we have seen three non-related cases. Though many providers are not knowledgeable about the dystrophy, its very unique appearance being cystic, epithelial and whorled—which, in my experience, is unlike any other corneal pathology—aids in its diagnosis.
| 1. Lisch W, Steuhl KP, Lisch C, et al. A new, band-shaped and whorled microcystic dystrophy of the corneal epithelium. Am J Ophthalmol. 1992;114(1):35-44. 2. Weiss JS, Møller HU, Aldave AJ, et al. IC3D Classification of Corneal Dystrophies—Edition 2. Cornea. 2015;34(2):117-59 3. Alvarez-Fischer M, Álvarez de Toledo J, Barraquer RI. Lisch corneal dystrophy. Cornea. 2005;24(4): 494-5. 4. Lisch W, Büttner A, Oeffner F, et al. Lisch corneal dystrophy is genetically distinct from Meesmann corneal dystrophy and maps to xp22.3. Am J Ophthalmol. 2000;130(4):461-8. 5. Lisch W, Wasielica-Poslednik J, Lisch C, et al. Contact lens-induced regression of Lisch epithelial corneal dystrophy. Cornea. 2010;29(3):342-5. 6. Salvador-Culla B, Alonso-Agesta M, Álvarez de Toledo J, et al. Combined keratectomy and localized limbal cauterization for treating Lisch epithelial corneal dystrophy. Cornea. 2019;38(2):243-5. |

