In just two years, the number of presbyopes in the United States is expected to climb to 123 million, or approximately three times the current population of California.1 This means that by 2020, an even greater population of fortysomethings will likely be sitting in your chair. While the list of treatment options for presbyopic patients continues to expand, soft multifocal contact lenses remain a top choice for many doctors.
Today’s multifocal designs are much improved from earlier generations, in part because the latest lenses are comprised of upgraded materials that don’t dry out by the end of the day. According to Justin Bazan, OD, of Park Slope Eye in Brooklyn, NY, dehydration routinely diminished optics in earlier multifocal designs.
Additionally, most of today’s multifocal lenses are available in single-use options, and their optics have been revamped to provide better vision based on how patients use their eyes, specifically with digital device use.
“Practitioners need to get excited about multifocal contact lenses and drop their baggage,” Dr. Bazan says. “Make multifocals a first option—and stick with the latest round of lenses—and you are going to be successful.”
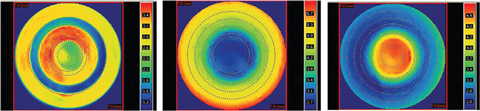 |
| At left is a simultaneous vision multifocal lens, which alternates between near and distance zones. In the center is a distance-center multifocal lens. At right is a near-center multifocal lens. Image: Robert L. Davis, OD |
Near or Far
Many of today’s popular multifocal soft contacts feature center-near designs, with the near focal power located in the middle of the lens and distance in the periphery.
Some available center-near designs include: Bausch + Lomb’s Ultra for Presbyopia and Biotrue OneDay for Presbyopia; Alcon’s Air Optix Aqua Multifocal and Dailies Total1 Multifocal; Johnson & Johnson Vision’s 1-Day Acuvue Moist Multifocal; and CooperVision’s Biofinity Multifocal (with the center-near design option).
Other soft multifocal lenses are based on a center-distance design. Here, the distance power is located in the middle of the lens and the near power is on the periphery. Common lenses with these designs include CooperVision’s Biofinity Multifocal (with the center-distance design option) and NaturalVue Multifocal 1 Day from Visioneering Technologies.
| The Perfect Fit 1. Make sure the patient isn’t over-minused. 2. Test for ocular dominance. If you’re fitting a multifocal patient and something isn’t going as planned, you may need to troubleshoot, and determining the dominant eye is key. Be sure to test for sensory dominance as opposed to sight dominance, Dr. Brujic says. Have the patient look at a target with both eyes open and place a +1.50 lens in front of each eye in succession (not simultaneously) to blur their vision, and ask which is better. The eye that doesn’t have the lens over it when the patient says they feel it’s better is the sensory-dominant eye. 3. Identify the patient’s goal. Dr. Brujic first asks the patient what he or she wants to achieve with a multifocal lens. “And ‘seeing up close’ isn’t specific enough,” he says. “If a patient responds they would like to see their cell phone better, that’s a specific goal.” Next, ask if there are other things the patient would like to be able to do better. “They might answer, ‘Yes, at work I want to be able to see my computer.’ Then we can ask, ‘How far is your computer away from you at work?’ so we know what type of distance we’re dealing with.” 4. Explain to the patient how and where multifocals will improve their vision—and when they might fall short. 5. Dive in and get lenses on the eyes. The sooner the conversation moves from concepts to trial fitting, the better. |
“In both lens designs, there is often a significant amount of asphericity, which allows them to have a smooth transition between each focal distance,” says Dave Anderson, OD, of Miamisburg Vision Care in Miamisburg, Ohio. “The biggest difference among all these lenses has to do with the emphasis on near or distance, as some perform better up close and some better at distance. Knowing this, I can choose what lens best suits the needs of each specific patient depending on their visual demands and their daily routines.”
The Duette Progressive Center Distance lens by SynergEyes—a hybrid design with a GP center and a soft lens “skirt”—is another newly available center-distance lens, with zone sizes ranging from 1.8mm to 4mm. According to the company, the lens is designed for patients experiencing challenges with distance vision and is also available in a near-center design.
While today’s simultaneous multifocal lens designs tout clear vision in all zones, they generally still impact distance vision to some degree, according to Brian Chou, OD, of EyeLux Optometry in San Diego. “I’m up front with my patients that this happens, but for many, multifocal contact lenses are still desirable because it gives them the benefit of improved near vision,” he says.
Tips From the Trenches
According to Robert L. Davis, OD, of Davis Eye Care Associates in Oak Lawn, IL, certain clinical pearls can help practitioners arrive at a particular lens design faster than a trial-and-error method. For example, if a patient is younger than 50 years old, Dr. Davis finds a distance-center lens often works better. Meanwhile, his patients 50 and older often do better in a near-center lens.
“If distance is in the center of the lens, then it is going to take real estate to get out to the necessary add power someone who is older is going to need,” he says. “If you use a near-center lens, the total near power is in the center, so you can control where the distance zone starts and make sure it is shorter than the pupil size.”
Today’s soft multifocal lenses can be customized, which can increase their success rate, Dr. Davis says. Some lens designs are available in multiple powers, and base curves, diameters and center and distance zones can be tailored to fit the patient’s needs.
According to Dr. Davis, the key to a successful fit is not the lens, but the patient. “What is controlling the patient’s ability to see is their pupil size,” he says. “You can try any lens design, but if there is a mismatch between the pupil size and the design, the patient isn’t going to be successful.”
For example, if a distance-center lens is 3mm in the center and everything outside of 3mm in near—and the patient’s pupil size is 2.5mm—the patient won’t be able to read up close because the pupil is smaller than where the reading zone starts.
“I’m asked all the time, ‘Is there one best lens?’ and my answer is, ‘If there was one best lens, there would be no others,’” Dr. Davis says. “Unless you use all the lenses, you’re going to limit your success because there is a place for them all. It’s just trying to find the match between the lens type and the patient.”
It is also prudent to read the patient’s reaction when they try on a soft multifocal lens, Dr. Davis says. “If a patient says to me, ‘I can’t see a thing in distance after I put a lens on,’ then I know I will need to increase the distance zone or decrease the near zone. Or if they say, ‘My distance is perfect, but I can’t read a thing close up,’ it’s not about power since I’ve already examined them—it’s about the real estate designated for near vision versus distance vision.”
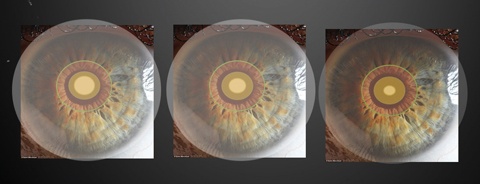 |
| Various multifocal zone sizes within a pupil. Image: Robert L. Davis, OD |
Mile Brujic, OD, of Premier Vision Group in Bowling Green, Ohio, routinely takes topography readings over the surface of a multifocal lens after it has been placed and centered on the eye. This gives him the ability to see where the optical zones are lined up over the patient’s physical line of sight, he says. “Prior to using topography over the surface of these lenses, there were some patients who did well and some who didn’t, and we really didn’t know why some were successful and others weren’t.”
Manufacturer fitting guides can also be helpful when fitting these patients. “It behooves all practitioners to put their egos aside and pull up the fitting guides,” says Dr. Bazan. “These are going to give you the best way to ensure your patient’s ideal outcome.”
Take a Test Drive
Patient misconceptions about multifocal contact lenses can be a barrier to finding the right lens, but putting on a trial lens during the exam can change patient perceptions, Dr. Davis says. Recently, after examining a 48-year-old female patient who wore a single vision distance disposable lens, Dr. Davis realized she needed a bifocal.
“Many of these patients don’t want to wear a bifocal because it’s a reminder they are getting older, and they don’t want any reminders,” says Dr. Davis. In this case, he put a multifocal trial lens on the patient without mentioning what it was, and the patient responded to her sharpened near and distance vision by calling Dr. Davis “a miracle worker.” Once the patient realized she could now see her phone and the letters on the distance acuity chart, Dr. Davis mentioned the lens he put on was a multifocal. “The patient then asked if she had to look at a particular spot, up or down, and I told her, ‘No, the lenses are center surrounding.’ Most patients think multifocal contacts are like spectacle multifocals, where distance is on top and reading is at the bottom of the lens.”
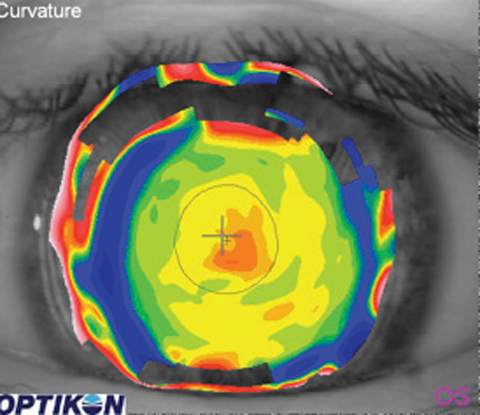 |
| A topography reading over a soft multifocal lens. The line of sight (represented by the cross) is located nasal to the near-center portion of the lens. Image: Mile Brujic, OD |
Best Candidates
Patient personalities—and expectations—should come into play when considering a fit for soft multifocal contacts. Listening to the patient’s needs and expectations is the most valuable indicator of success when fitting multifocals, says Glenda Secor, OD, of Huntington Beach, CA.
Additionally, she says all presbyopic patients should be informed of the multifocal options including contact lenses. “Highly motivated patients are the easiest. Early presbyopes and hyperopes are generally great candidates.”
It’s also important to remember the goal of using a multifocal lens is not to get the patient crystal clear vision, but functional vision, says Dr. Chou. “The OCD patients who are comparing the vision in their right eye with their left eye are generally not the types of patients to get into a multifocal contact,” he says.
Additionally, you may want to reconsider perfectionist patients who will compare their multifocal contact lens vision with the most updated progressive glasses, Dr. Chou adds. Instead, the best patients are the ones who will benchmark their vision through a multifocal contact lens against their uncorrected vision. “I tell patients that their vision with a multifocal lens is going to be way better compared with their naked eye, but it’s not going to approach what they would get with updated glasses, which is honest,” says Dr. Chou. “It’s always better for practitioners to under-promise and over-deliver.”
For Dr. Anderson, the selection process for current contact lens wearers begins with understanding what a patient does with their eyes and how much of an issue the near is for them. “If someone is noticing a slight blur at the end of the day on medicine bottles in low light, I will tell them they are going to need a multifocal lens in the near future,” he says. “For current wearers who have just started trying over-the-counter readers or those who are noticing their phones are always blurry, I will nearly always push towards a multifocal contact lens.”
| What to Charge? On the other hand, Dr. Brujic advises practitioners to set multifocal fitting fees higher than spherical lens fitting fees. “It takes more knowledge from the practitioner to be able to effectively and efficiently fit these lenses,” he says. Dr. Anderson agrees, citing the additional time and effort required to successfully fit multifocal lenses. “I charge accordingly, and this is typically 2.5 times what I base my spherical contact lens fees on,” he says. “Not only do they require more follow up typically, these patients also need more coaching while wearing the lens.” |
When evaluating prospective new wearers, Dr. Anderson focuses almost entirely on what they do with their eyes. If a patient does mostly distance tasks, they may be quicker to notice the flaws of multifocal contacts, but if they work up close all day, they will be quicker to notice the benefits.
Accentuate the Positive
Managing patient expectations doesn’t end after the initial fit, however.
Something as simple as word choices can make a difference in patient perception. Dr. Chou refers to the second office visit as a “progress visit” rather than a “follow-up.” This reinforces the value of the appointment for the patient. Often, practitioners with lower success in prescribing multifocal lenses treat subsequent appointments like medical visits, Dr. Chou adds. “The first question they ask is, ‘Are you having any problems?’ The better questions is, ‘How are you enjoying your freedom from glasses?’”
Practitioners who adopt the medical model for multifocal lens visits generally also make the mistake of checking each eye individually first, and then having the patient read the smallest letter on the screen to get to the measurement endpoint as quickly as possible, Dr. Chou says. “That psychologically puts doubt in the mind of the patient because multifocal patients usually don’t see the 20/20 line crystal clear.” Instead, he believes practitioners should ask positive questions, check visual acuity first binocularly with both eyes open and start with one of the largest letters that the patient couldn’t see uncorrected prior to the treatment.
On the Horizon
One promising multifocal working its way through the pipeline is an accommodating contact lens from the Vistakon division of Johnson & Johnson Vision.2-4 “It sounds remarkable,” says Dr. Chou. “The lens would change focus like an autofocus camera.”
In a similar vein, Verily and Alcon are working to develop a smart, accommodating soft contact lens that contains tiny integrated circuits, sensors and wireless communication capabilities for self-contained wireless sensing on the surface of the eye.5
Improvements more likely in the near-term will expand the range of candidates who can try multifocal lenses. “While our spherical patients have a plethora of options currently out on the market, our astigmatic patients do not enjoy such options,” Dr. Bazan says. “However, there are innovations in multifocal technology coming up and in a couple of years they will have some.”
Overall, soft multifocal contact lenses have come a long way since their introduction, and that should encourage doctors to embrace these designs when dealing with presbyopic patients. “Everyone’s a potential candidate,” Dr. Bazan stresses. “Follow the fitting guides and drop your baggage. The new lenses are awesome.”
1. Market Scope. Global Presbyopia-Correcting Surgery Market Report. April 2012. |

