 |
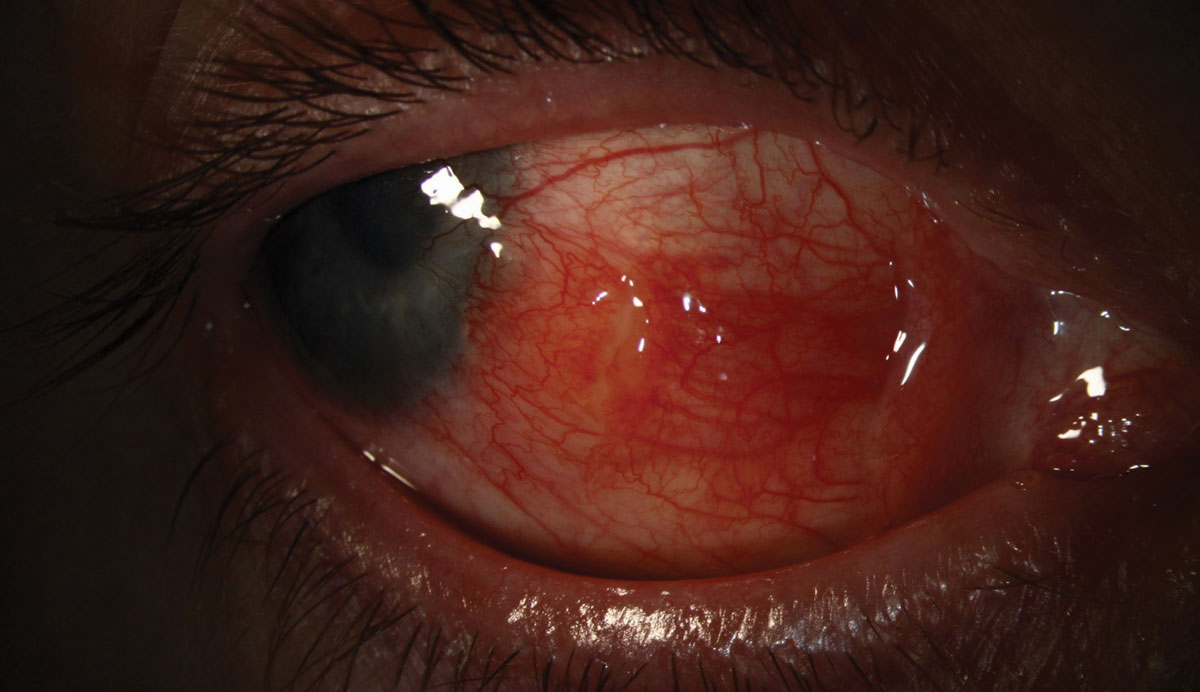
This patient is a 46-year-old male who suffered an alkaline burn to the right eye that resulted in severe limbal stem cell deficiency, corneal neovascularization and scarring, as well as recurrent erosions and pain. He was fit into a scleral device for pain relief. After several years of successful wear, he reported to our office with complaints of rapid-onset redness and irritation adjacent to the lens edge. He was diagnosed with a pyogenic granuloma.
Prednisolone was prescribed, which improved but did not resolve the granuloma. Surgical resection was discussed, but because he would need to be without the comfort-giving scleral device until healed, he opted for impression technology using an elevation-specific scleral design. An impression of the ocular surface was obtained using a polyvinylsiloxane mold and a custom scleral device was designed to shield and cover the granuloma. A few months later, the granuloma had completely resolved.
A pyogenic granuloma is a mix of inflammatory cells, blood vessels and conjunctival tissue. It is commonly seen after ocular surface surgeries when there is a chronic irritation, such as a scleral lens or exposed suture, or in inflammatory conditions such as Steven-Johnson syndrome. Histologically, they are either inflammatory or fibrotic lesions.1
Inflammatory lesions, characterized by proliferation of capillaries and inflammatory cells, are mainly associated with bulbar conjunctiva surgery or injury. Fibrotic granuloma, characterized by loose fibrous stroma, is mainly associated with chronic chalazion on the tarsal conjunctiva.2
Pyogenic granuloma must be differentiated from malignant lesions. A major distinguishing factor is timing. Granulomas develop rapidly, while lesions such as squamous cell carcinoma have a slower onset.
The main treatment includes topical steroids QID for one to two weeks. If this does not resolve the lesion, surgical excision is generally recommended. However, other treatments have been prescribed: topical 0.5% timolol BID for three weeks, cryosurgery and chemical cauterization are potential options. Avoidance of the inciting factor is also effective at resolving the lesion.
 |
| Click photo to enlarge. |
1. Wu D, Qian T, Nakao T, et al, Medically uncontrolled conjunctival pyogenic granulomas: correlation between clinical characteristics and histological findings. Oncotarget. 2017 Jan 10; 8(2): 2020–2024. 2. Oke I, Alkharashi M, Petersen RA, Ashenberg A, Shah AS. Treatment of ocular pyogenic granuloma with topical timolol. JAMA Ophthalm. 2017 Apr 1;135(4):383-385. |

