 |
Managing Presbyopia with Multifocal Contact Lenses
Effectively using this modality to treat this condition benefits both patients and providers.
By Erin Rueff, OD, PhD
Release Date: November 15, 2023
Expiration Date: November 15, 2026
Estimated Time to Complete Activity: 2 hours
Jointly provided by Postgraduate Institute for Medicine (PIM) and Review Education Group.
Educational Objectives: After completing this activity, the participant should be better able to:
Select the right multifocal contact lens for their presbyopic patient.
Successfully fit their patients with multifocal contact lenses.
Educate patients on the benefits of multifocal contact lenses for presbyopia.
Effectively manage presbyopic patients with multifocal contact lenses.
Target Audience: This activity is intended for optometrists who want to use this modality to treat this condition.
Accreditation Statement: In support of improving patient care, this activity has been planned and implemented by PIM and the Review Education Group. PIM is jointly accredited by the Accreditation Council for Continuing Medical Education, the Accreditation Council for Pharmacy Education and the American Nurses Credentialing Center to provide CE for the healthcare team. PIM is accredited by COPE to provide CE to optometrists.
Faculty/Editorial Board: Erin Rueff, OD, PhD
Credit Statement: This course is COPE approved for 2 hours of CE credit. Activity #127150 and course ID 87981-CL. Check with your local state licensing board to see if this counts toward your CE requirement for relicensure.
Disclosure Statements: PIM requires faculty, planners and others in control of educational content to disclose all their financial relationships with ineligible companies. All identified conflicts of interest are thoroughly vetted and mitigated according to PIM policy. PIM is committed to providing its learners with high-quality, accredited CE activities and related materials that promote improvements or quality in healthcare and not a specific proprietary business interest of an ineligible company.
Those involved reported the following relevant financial relationships with ineligible entities related to the educational content of this CE activity: Authors—Erin Rueff, OD, PhD. Managers and Editorial Staff—The PIM planners and managers have nothing to disclose. The Review Education Group planners, managers and editorial staff have nothing to disclose.
 |
A patient’s satisfaction with their correction will determine if they stick with their multifocal lenses. Click image to enlarge. |
Presbyopic contact lens wearers offer incredible opportunities for any contact lens practice. Depending on the practice setting, patients in the presbyopic age range may make up more than half of all soft contact lens prescriptions. Even though presbyopic wearers take up the near majority of the contact lens market, only about 60% of contact lens wearers in the presbyopic age range are actually wearing a contact lens that addresses both their near and distance visual needs.1
There are different possibilities when considering how to address the unique visual demands of a presbyopic contact lens wearer, but as technology continues to improve, it is apparent that multifocal contact lenses are the right option for the majority of presbyopic soft contact lens wearers. This article will explain why multifocals are the best presbyopic soft contact lens option, describe how soft multifocal contact lenses work and present strategies that will lead to successful multifocal lens fittings.
Weighing the Presbyopic Options
A presbyopic soft contact lens wearer has many options when it comes to correcting their vision at all distances. While single vision contact lenses with overlay reading or distance glasses might seem like the easiest option, this choice does not allow an existing contact lens wearer to remain spectacle-free. When choosing a contact lens option for a presbyope who wants to address both distance and near vision, eye care providers typically consider monovision or multifocal modalities.
Monovision is a presbyopic correction strategy that uses single vision contact lenses to correct one eye for distance vision and the other eye for a specific near working distance, inducing anisometropia.2 When looking at distance, the brain effectively suppresses the near-corrected eye, and vice versa. In theory, this suppression results in binocular acuity that matches the better seeing eye for a particular visual task.3 For the majority of patients, the “dominant” eye is corrected for distance while the “non-dominant” eye is corrected for near vision.2
Because single vision, non-multifocal soft contact lens options were the first commercially available, monovision was the first non-spectacle strategy used to correct presbyopia in contact lens wearers. As multifocal options began to enter the contact lens market, early designs often suffered from reduced vision at all distances due to the manipulation of spherical aberrations (see later section for a detailed description of multifocal optics). Spherical aberrations can degrade the image on the retina, and this image degradation has been reported to cause blur, decreased contrast sensitivity and glare.4-12
Monovision is preferred by some prescribers because it provides crisp vision at each corrected distance.13 There is a perception that this presbyopic modality is simpler and requires less fitting time.14 The anisometropia induced by this correction type, however, reduces stereoacuity, especially with high add powers.4,5,15,16 Due to this reduction in depth perception, monovision is prohibited in certain professions like piloting, professional driving and some competition sports.2 Additionally, the two corrected distances typically provide clear images, but visual targets within those distances may result in reduced acuity.
Multifocal contact lenses theoretically provide clear vision at an infinite number of points from distance, to intermediate to near. Historically, multifocal designs have been described as requiring the patient to “sacrifice” clear vision at one distance in order to achieve acceptable vision at another. As technology has advanced, however, more recent multifocal designs result in distance and near vision that is similar to monovision and also do not affect stereoacuity and depth perception.4,5
 |
|
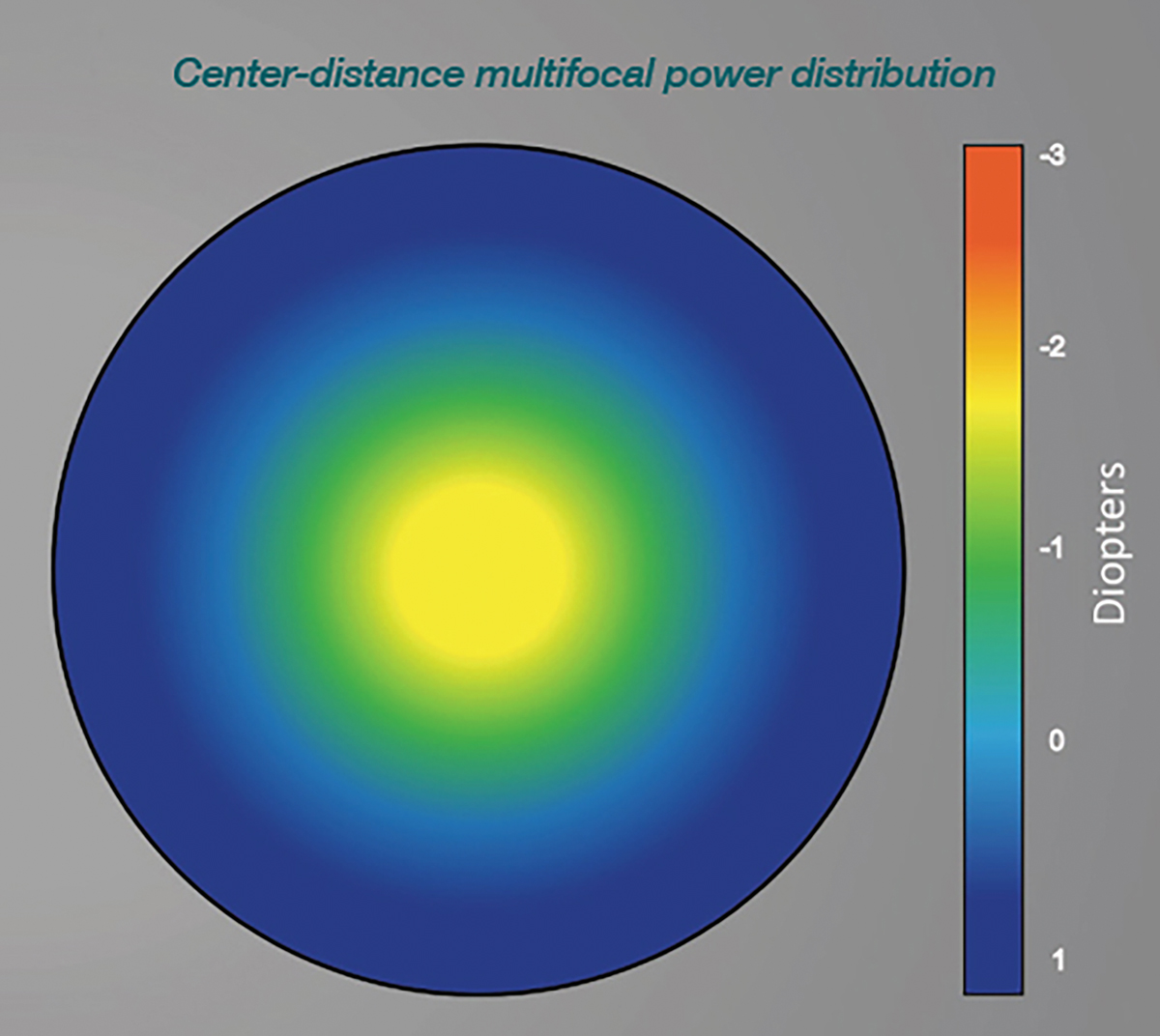
Center-distance multifocal contact lens designs have been suggested to be optimal for early presbyopes and/or presbyopes with high distance vision demands, but center-near designs are the most common option on the market today. Photo: Keyur Savla. Click image to enlarge. |
Multifocals or Monovision?
As multifocals have evolved and newer designs have emerged that address the image degradation issues described above, clinicians are often left with the task of choosing a monovision or multifocal option for presbyopic contact lens wearers.
Studies using various multifocal designs have compared multifocals to monovision to determine which modality works best. A 2003 investigation refit existing monovision wearers into a multifocal and showed high-contrast visual acuity was the same at all distances, but stereoacuity was better with the multifocal.17 Subjective ratings for various distances and tasks were better for the multifocal.17 One study found that high-contrast visual acuity was no different for either correction and stereoacuity was improved with multifocals.4 An impressive 76% of wearers preferred the multifocal to monovision in this trial.4 Other trials have similarly reported better stereopsis with multifocals compared to monovision.5,7,18,19
Other studies have reported more mixed visual acuity results when comparing the two correction types. Some research has reported reduced vision with multifocals only in low-light and/or low-contrast environments, while others suggest objective visual assessment is better with monovision at all distances.4,5, 7,15,17,20 A more recent study reported that early presbyopes corrected with monovision frequently accommodated with the distance-corrected eye, leaving the near eye with myopic defocus and reduced acuity at near.21
The most important factor when assessing the success of any presbyopic contact lens modality is the patient's subjective response. A patient’s opinion and satisfaction with their correction is the factor that will determine if they remain in that correction. When considering subjective assessments of multifocal and monovision contact lens designs, patients prefer simultaneous vision multifocals to monovision. In the studies mentioned above, 51% to 76% of patients preferred multifocals to monovision.4,7 Subjective ratings of a multifocal were higher for most tasks and especially for changing focus.4,7,15,17
These findings show that objective visual assessments (i.e., visual acuity measures) of presbyopic contact lens options may not be as valuable as subjective responses. A patient’s opinion of the contact lens outside of the exam lane and into their everyday life and activity is likely more important than what line they can read on their eye care provider’s carefully calibrated visual acuity chart. It has been suggested that, even if the visual acuity measure is not as good with a multifocal contact lens, the subjective performance of the multifocal in the real world makes the wearer prefer a multifocal design to monovision.7 Multifocals, therefore, should be the first-considered option when fitting a presbyopic soft contact lens wearer.
A Review of Multifocal Optics
This contact lens option has undergone many changes and technological advances over the last few decades. It is easy to get overwhelmed by the optical jargon that accompanies each individual multifocal design, but understanding multifocal optics does not have to be overly complicated. Most modern soft multifocals on the market employ some sort of simultaneous image optical design.
Simultaneous image multifocals, in general, position distance and near powers over the pupil at the same time. The optical zone that centers over the pupil contains multiple powers that correspond to a range of near and far distances.22 The lens simultaneously focuses multiple images on the retina and the patient attends to the clearest images based on the visual task.23
Multifocal contact lenses using simultaneous image optics include diffractive, concentric, aspheric and extended depth of focus designs.22,24 Concentric designs have small annular zones that contain distance and near power.13 Diffractive designs focus distance images by refraction of light and near images by diffraction.25 Extended depth-of-focus designs manipulate the magnitude and sign of higher order spherical aberrations to increase depth of focus (similar to aspheric designs described below) in a manner that will improve presbyopic near and intermediate vision without compromising distance vision as much as previous aspheric designs.24,26 Diffractive designs are not currently commercially available and concentric designs only exist in older, less used options.6 The majority of extended depth-of-focus multifocal contact lenses currently on the market are marketed for myopia management, not presbyopia.27,28
While understanding that there are different types of simultaneous image multifocals is helpful, multifocal optics can be easier understood by recognizing that the most prevalent simultaneous multifocals available commercially today use aspheric designs. Instead of having near or distance “zones” like a translating gas permeable contact lens or concentric multifocal design, aspheric designs use spherical aberration to increase the depth of focus and “pseudo-accommodate” for the lacking true accommodation in presbyopes.29,30 Similar to how a PAL spectacle lens provides clear vision at more distances than a flat top bifocal, an aspheric multifocal design will offer a similar range of clear vision compared to the distinct distances offered by a translating or concentric contact lens design.
Aspheric multifocals are designed with center-near or center-distance power orientations. Center-near designs add negative spherical aberration and center-distance designs add positive spherical aberration to the center of the lens.31 The change in aberrations results in a power profile that gradually changes from near to distance power or vice versa.31 This increased depth of focus, therefore, introduces simultaneous distance and near images on the retina.32
Center-near designs are most common commercially. Because of miotic pupil changes that occur when accommodation is stimulated and the age-related decrease in pupil size, maximal near vision is achieved when the near correction is in the middle of the optical zone.33,34 Center-distance designs have been suggested to be optimal for early presbyopes and/or presbyopes with high distance vision demands. Center-distance designs are also used to prevent progression of myopia in children.35,36
 |
|
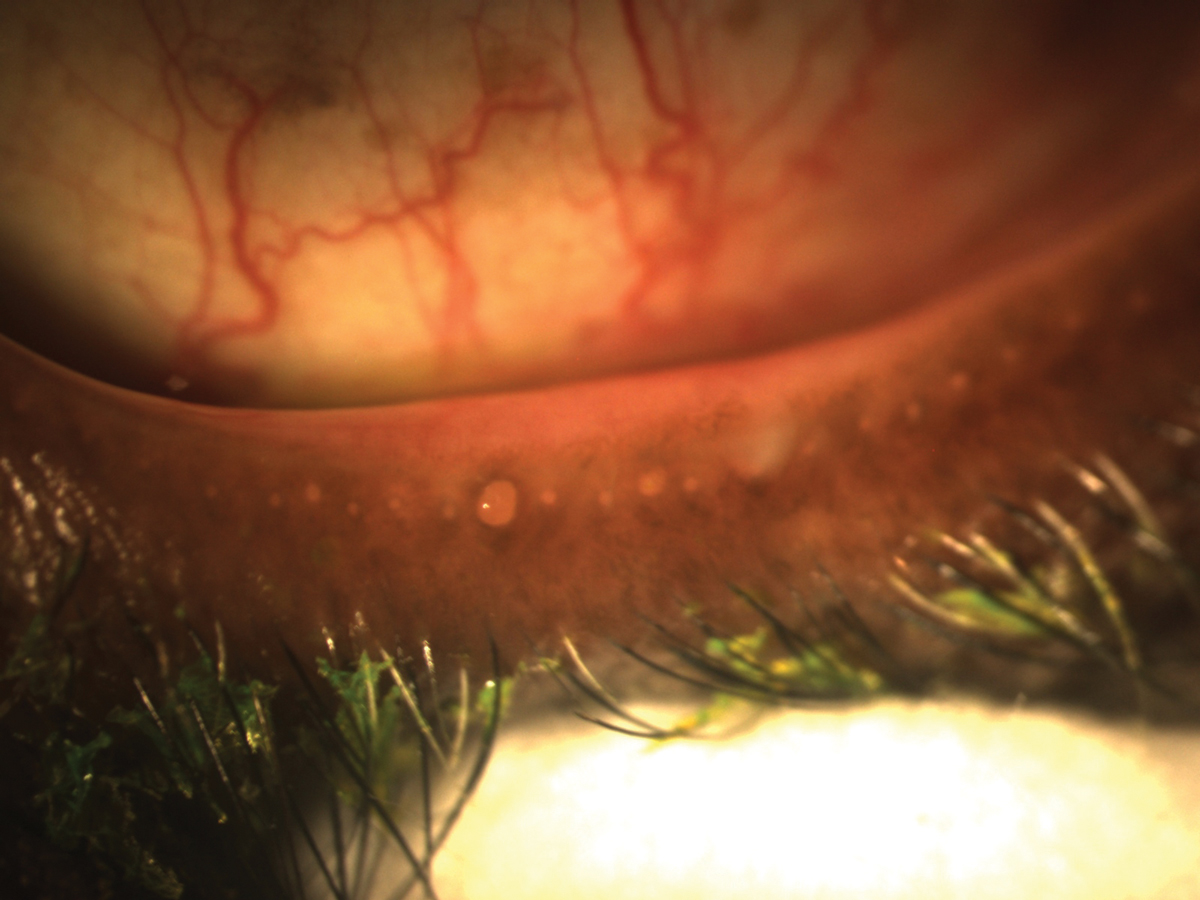
Manage existing meibomian gland disease or signs of dry eye throughout the fitting process to ensure that any associated symptoms do not interfere with comfort or visual outcomes of the lenses. Photo: Doan Huynh Kwak, OD. Click image to enlarge. |
Starting Successful Multifocal Fittings
Now that you recognize the importance of choosing a multifocal option for your presbyopic soft contact lens wearers, it is important to understand the best approaches for initiating and troubleshooting multifocal contact lens fits. The remaining sections will focus on strategies that will lead you to success with multifocal contact lens fitting.
Before even thinking about lens brand or parameter availability, it is imperative to collect updated and accurate refractive data first. When a presbyope is in the exam chair, it can be tempting to assume that their refractive error is stable and unlikely to have changed since the last exam. It is vital to acknowledge, however, that refractive error can still fluctuate in presbyopic years and small power changes (0.25D to 0.50D) can have a big impact on a patient’s subjective experience with a multifocal.
Additionally, it is common for early presbyopes to “drop minus” or appear to become less myopic as they enter presbyopia, likely because they were over-corrected in their pre-presbyopic years. Add power also changes with time, so verifying optimal add power at the beginning of each fitting is key. Make sure you begin the multifocal fitting with current, balanced, vertexed refractive data so you are most likely to pull the correct lens power on the first try.
Next, perform a careful ocular health assessment. Presbyopic vision does not occur in a vacuum; ocular health issues like dry eye, pre-existing retinal conditions and ocular medications might influence how the contact lens interacts with the eye and/or what the final visual outcome is. Acknowledging any pre-existing ocular conditions and managing them before the fit can be helpful. For example, existing meibomian gland disease or signs of dry eye could be managed throughout the fitting process to ensure that symptoms associated with these conditions do not interfere with comfort or visual outcomes of the lenses.
Finally, it is time to choose a lens. It might feel daunting to decide which lens to start with and how to initiate the most effective and efficient fitting process. If you are new to soft multifocal contact lenses, consider starting with one brand or one manufacturer first. Each multifocal design has its own unique nuances, so starting with and sticking to one design will allow you to get comfortable with the lens design and how it can best serve your patients.
Most major contact lens manufacturers maintain the same multifocal optical design across different brands and replacement schedules within their portfolio. This means that you often will have a daily, monthly and/or biweekly replacement option with the same multifocal design, allowing you to use the same optical design for patients with different needs and refractive errors.
Fitting and Follow-Up
For every multifocal currently on the market, there is a detailed, step-by-step fitting guide developed by the manufacturer that is intended to optimize the chance for initial success with that unique multifocal design. In the past, multifocal fitting sets may have had little to no instruction. Eyecare providers were left to develop fitting strategies and rationales on the spot to determine how to address their patient’s visual needs.
Since those early days of multifocal contact lenses, manufacturers have realized that each individual design requires unique steps to achieve good vision at all distances. Fitting guides, therefore, have been developed by testing each design on large samples of patients. Through the fitting guide development, the manufacturer determines what the most effective strategies are for choosing the initial lenses and troubleshooting when patients have visual complaints at various distances. This is incredibly helpful to come up with several logical ways to address patients' specific complaints. The fitting guide will describe the solution that is most likely to address the issue and lead to success. This expedites the fitting process and ensures more patients will succeed with the lenses.
Once you have trialed the initial lens suggested by the fitting guide, consider sticking with that combination unless vision is very unsatisfactory at distance or near. If binocular vision with the lenses is satisfactory at most distances, acknowledge that vision will likely improve with adaptation (see below) and plan for a follow-up visit to check back in after adaptation. If vision is quite bothersome at one distance or another, however, use the fitting guide to adjust powers appropriately.
 |
|
Multifocals should be the first considered option when fitting a presbyopic soft contact lens wearer. Photo: Alex Nixon, OD, MS, and Erin Rueff, OD, PhD. Click image to enlarge. |
Establish Expectations, Educate Effectively
The most important step of a successful multifocal contact lens fitting is concise, clear, optimistic patient education. While multifocal contact lens optics have improved and can provide excellent vision at all distances, the complex optics that simultaneous aspheric multifocals introduce can take time to adapt to.
Recent research has shown that multifocal visual acuity and symptoms associated with light disturbances improve over a two-week time period of continued lens wear.19,37 This means that, as the patient continuously wears the lenses, the brain and visual system are able to learn how to use the unique optics of the multifocal. It has been suggested that eye care providers will have more success with multifocal fittings if they prepare their patients for this adaptation process.19,37
Effective multifocal education does not have to involve excessive amounts of chair time. Explain how the lenses work in easy-to-understand language and let the patient know that once they have adapted to the lenses, more meaningful changes and alterations can be made to address any issues they have. Consider the following expectation education example:
“These contact lenses focus multiple images on the back of your eye at the same time, so it will take a little while for your brain to figure out how to use this new lens. It is normal for vision to seem different or slightly altered during the first days of lens wear. Most patients experience improved vision as they continue to wear the lenses. Once you have adapted to the lenses, I can make more meaningful adjustments to the lens power. I am looking forward to hearing your impressions of the lenses at the follow-up visit and refining anything that might need adjusting.”
This short explanation helps the patient understand the lenses, lets them know what to expect during the adaptation process, and instills confidence and optimism that you can address any issues they have after initial adaptation. This quick education will have a lasting impact on the patient’s attitude toward the overall fitting process, improving your chance for success.
Takeaways
Presbyopic contact lens wearers have many options for correcting their unique visual needs. The evolution of lens technology over the last several decades has led to optical designs that perform well for most patients. In 2023, we no longer need to settle for overlay spectacles or monovision. Multifocal contact lens designs offer the best option for clear vision at all distances while maintaining stereopsis.
Successful presbyopic soft contact lens wear begins with an eye care provider who is willing and eager to prescribe a multifocal contact lens design, embrace the manufacturer’s recommendations for fitting that lens and thoughtfully educate the patient about the fitting process.
Dr. Rueff is an associate professor and chief of cornea and contact lens services at the Southern California College of Optometry at Marshall B. Ketchum University (MBKU). Before MBKU, she received her optometry degree, completed the Cornea and Contact Lens Advanced Practice Fellowship and earned a PhD in Vision Science at the Ohio State University. She is a fellow of the American Academy of Optometry and a diplomate of its Cornea, Contact Lens and Refractive Surgeries Section. Dr. Rueff’s clinical and research interests include contact lens discomfort, dry eye, presbyopic contact lenses and keratoconus.
1. Morgan PB. International contact lens prescribing in 2022. CL Spectrum. 2023;38:28-35. 2. Seijas O, Gomez de Liano P, Gomez de Liano R, et al. Ocular dominance diagnosis and its influence in monovision. Am J Ophthalmol. 2007;144(2):209-16. 3. Schor C, Erickson P. Patterns of binocular suppression and accommodation in monovision. Am J Optom Physiol Opt. 1988;65(11):853-61. 4. Richdale K, Mitchell GL, Zadnik K. Comparison of multifocal and monovision soft contact lens corrections in patients with low-astigmatic presbyopia. Optom Vis Sci. 2006;83(5):266-73. 5. Gupta N, Naroo SA, Wolffsohn JS. Visual comparison of multifocal contact lens to monovision. Optom Vis Sci 2009;86(2):E98-105. 6. Perez-Prados R, Pinero DP, Perez-Cambrodi RJ, Madrid-Costa D. Soft multifocal simultaneous image contact lenses: a review. Clin Exp Optom. 2017;100(2):107-27. 7. Woods J, Woods C, Fonn D. Visual performance of a multifocal contact lens vs. monovision in established presbyopes. Optom Vis Sci. 2015;92(2):175-82. 8. Garcia-Lazaro S, Ferrer-Blasco T, Madrid-Costa D, et al. Visual performance of four simultaneous-image multifocal contact lenses under dim and glare conditions. Eye Contact Lens. 2015;41(1):19-24. 9. Fisher K, Bauman E, Schwallie J. Evaluation of two new soft contact lenses for correction of presbyopia: the focus progressives multifocal and the Acuvue bifocal. Int Contact Lens Clin. 2000;26(4):92-103. 10. Guillon M, Maissa C, Cooper P, et al. Visual performance of a multi-zone bifocal and a progressive multifocal contact lens. CLAO J. 2002;28(2):88-93. 11. Harris MG, Sheedy JE, Gan CM. Vision and task performance with monovision and diffractive bifocal contact lenses. Optom Vis Sci. 1992;69(8):609-14. 12. Sheedy JE, Harris MG, Bronge MR, et al. Task and visual performance with concentric bifocal contact lenses. Optom Vis Sci. 1991;68(7):537-41. 13. Back A, Grant T, Hine N. Comparative visual performance of three presbyopic contact lens corrections. Optom Vis Sci. 1992;69(6):474-80. 14. Bennett ES. Contact lens correction of presbyopia. Clin Exp Optom. 2008;91(3):265-78. 15. Woods J, Woods CA, Fonn D. Early symptomatic presbyopes-what correction modality works best? Eye Contact Lens. 2009;35(5):221-6. 16. Kirschen DG, Hung CC, Nakano TR. Comparison of suppression, stereoacuity and interocular differences in visual acuity in monovision and Acuvue bifocal contact lenses. Optom Vis Sci. 1999;76(12):832-7. 17. Situ P, Du Toit R, Fonn D, Simpson T. Successful monovision contact lens wearers refitted with bifocal contact lenses. Eye Contact Lens. 2003;29(3):181-4. 18. Sivardeen A, Laughton D, Wolffsohn JS. Randomized crossover trial of silicone hydrogel presbyopic contact lenses. Optom Vis Sci. 2016;93(2):141-9. 19. Fernandes PR, Neves HI, Lopes-Ferreira DP, et al. Adaptation to multifocal and monovision contact lens correction. Optom Vis Sci 2013;90(3):228-35. 20. Kang P, McAlinden C, Wildsoet CF. Effects of multifocal soft contact lenses used to slow myopia progression on quality of vision in young adults. Acta Ophthalmol. 2017;95(1):e43-53. 21. Almutairi MS, Altoaimi BH, Bradley A. Accommodation in early presbyopes fit with bilateral or unilateral near add. Optom Vis Sci. 2018;95(1):43-52. 22. Charman WN. The eye in focus: accommodation and presbyopia. Clin Exp Optom. 2008;91(3):207-25. 23. Charman WN. Developments in the correction of presbyopia i: spectacle and contact lenses. Ophthalmic Physiol Opt. 2014;34(1):8-29. 24. Tilia D, Bakaraju RC, Chung J, et al. Short-term visual performance of novel extended depth-of-focus contact lenses. Optom Vis Sci. 2016;93(4):435-44. 25. Toshida H, Takahashi K, Sado K, et al. Bifocal contact lenses: history, types, characteristics and actual state and problems. Clin Ophthalmol. 2008;2(4):869-77. 26. Tilia D, Munro A, Chung J, et al. Short-term comparison between extended depth-of-focus prototype contact lenses and a commercially-available center-near multifocal. J Optom. 2017;10(1):14-25. 27. Misight 1 Day (omafilcon a) soft (hydrophilic) contact lenses for daily wear – P180035. US Food & Drug Administration. www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpma/pma.cfm?id=P180035. Accessed October 16, 2023. 28. Redefine their tomorrow. VTI Vision. vtivision.com/practitioner/myopia/. Accessed October 16, 2023. 29. Altoaimi BH, Almutairi MS, Kollbaum P, Bradley A. Accommodative behavior of eyes wearing aspheric single vision contact lenses. Optom Vis Sci. 2017;94(10):971-80. 30. Kollbaum PS, Bradley A, Thibos LN. Comparing the optical properties of soft contact lenses on and off the eye. Optom Vis Sci. 2013;90(9):924-36. 31. Montes-Mico R, Madrid-Costa D, Dominguez-Vicent A, et al. In vitro power profiles of multifocal simultaneous vision contact lenses. Cont Lens Anterior Eye. 2014;37(3):162-7. 32. Ruiz-Alcocer J, Madrid-Costa D, Radhakrishnan H, et al. Changes in accommodation and ocular aberration with simultaneous vision multifocal contact lenses. Eye Contact Lens. 2012;38(5):288-94. 33. Begun JA. Mechanisms of accommodation. Optom Vis Sci. 1993;70(8):694-5. 34. Wang B, Ciuffreda KJ. Depth-of-focus of the human eye: theory and clinical implications. Surv Ophthalmol. 2006;51(1):75-85. 35. Walline JJ. Myopia control: a review. Eye Contact Lens. 2016;42(1):3-8. 36. Walline JJ, Greiner KL, McVey ME, Jones-Jordan LA. Multifocal contact lens myopia control. Optom Vis Sci. 2013;90(11):1207-14. 37. Fernandes P, Amorim-de-Sousa A, Queiros A, et al. Light disturbance with multifocal contact lens and monovision for presbyopia. Cont Lens Anterior Eye. 2018;41(4):393-9. |

