  |
A 49-year-old male presents for his annual contact lens evaluation. The patient habitually uses orthokeratology (ortho-K) lenses and reports excellent distance vision with 20/20 entering visual acuity in both right and left eyes. He reports wearing his lenses for eight hours the night prior to his examination, though he often skips up to three nights, with no reported adverse side effects related to overnight contact lens wear. He does, however, report near vision blur the day after wearing his lenses overnight and his near visual acuity with both eyes open was 20/40. He also reports that he has to do very fine, meticulous near work, as he is a handyman. On days when he did not wear his lenses the night prior, he reports comfortable near vision. During a separate visit, he had not worn his lenses for three nights and his manifest refraction was -0.50 Sph OD and -0.50 Sph OS with a +1.25 add OU. Prior to ortho-K wear, his refraction was -0.75 -1.00x154 OD and -0.75 -1.00x0.35 OS. He wishes to continue wearing ortho-K but improve his near vision.
Considerations
Here, we highlight our thought processes and consider how we would proceed:
Dr. Pfeifer: Patients who are developing presbyopia provide a unique challenge, in that they’re losing part of their functional vision in a normal, expected way. For eyecare practitioners, this is something that is very mundane, but for the patient, their world is changing. Giving the appropriate weight to their concern, while talking about options for improvement, will allow them to feel heard, but also hopeful. Patients in ortho-K, especially long-time wearers, may struggle with this insidious near blur as they have become accustomed to not wearing correction throughout the day. This can amplify the burden of wearing readers and leave the patient feeling dissatisfied.
Given this, my preference would be to incorporate a +1.00D to +1.50D “boost” into the nondominant eye’s lens to give a usable range of vision. If the patient is not amenable to modifying his lenses or his wear schedule, informing him that the near vision blur will only increase as time passes is essential. He will likely begin to need supplemental near vision glasses for days following lens wear and distance vision glasses for tasks like driving on days when he skipped lens wear. He also has the option of wearing multifocal soft or specialty contact lenses on days after he skips ortho-K wear. Supplementation with pharmaceuticals targeted at improving near vision in presbyopic patients could also be considered. Ultimately, the patient is going to dictate how he approaches presbyopia once he is aware of all the realistic options. If he decides to discontinue ortho-K wear, a multitude of soft or specialty extended depth-of-focus or multifocal options are a possible solution going forward.
Dr. Su: In this case, the patient has excellent distance vision with ortho-K but struggles with near vision, and he often skips wearing the lenses for three nights at a time. It’s important to clarify whether these lapses are accidental, which coincidentally improves his near vision, or if they are deliberate efforts to enhance his close-up vision. Understanding the patient’s behavior and expectations is crucial, as well as setting realistic expectations. If he wants to maintain his 20/20 distance vision while improving his near vision for work and not have the need to wear reading glasses, a blended vision approach could be beneficial. I find that adding a +1.25D or +1.50D add in the nondominant eye often successfully meets most patients’ needs without significantly reducing stereoacuity. However, to test this, I’d recommended a washout period and trial this with soft lenses for about a week.
Dr. Noyes: Though I don’t do ortho-K in my clinic, creative applications such as over-spectacles, under-correction and monovision could do well for this patient. Too many practitioners conceptualize ortho-K as being “kids only,” and this case demonstrates widening its use in a safe and effective way.
Dr. Gelles: There are a few considerations to be made here. First is his occupation: the obvious option is for him to use an occupation pair of glasses at work; it will give him a near add, but more importantly, double as a pair of safety glasses.
If we are looking specifically at options to modify his current ortho-K wear, we must keep in mind the patient is myopic and reports that under-correction from the ortho-K makes him happy at work. An easy fix could be to reduce the target power to give a little less myopic correction, allowing him to have clearer near vision. If near work is 90% of his need, over-spectacles with the rest of the myopic correction can be used as needed.
A classic line from the podium is, “Orthokeratology is inherently multifocal,” as the correction causes increased spherical aberration similar to a center distance multifocal contact lens. A smaller optic zone will give more multifocal effect by pushing the reverse zone inward, increasing spherical aberration and thus providing more depth-of-focus. An alternative to that is the use of blended vision, where the dominant eye is fully corrected and the non-dominant eye is corrected to -1.25D. The issue here is that detailed near work generally needs good binocularity and this is likely not the best option.
If he likes clearer vision at distance on the weekends, in this case, having two pairs of ortho-K lenses might offer the best solution: one pair for fully corrected distance worn on Friday and Saturday night for a distance task-heavy weekend, and the other worn Sunday through Thursday with reduced target correction for his occupational needs.
Ultimately, if the patient is happy and healthy, why change? The cycle seems to be meeting his needs, so let him keep doing what he’s doing, get him a pair of distance spectacles for when he’s under-corrected and keep monitoring his health. If he’s considering discontinuing ortho-K for convenience, a refractive lens exchange with a premium intraocular lens could satisfy his needs.
 |
|
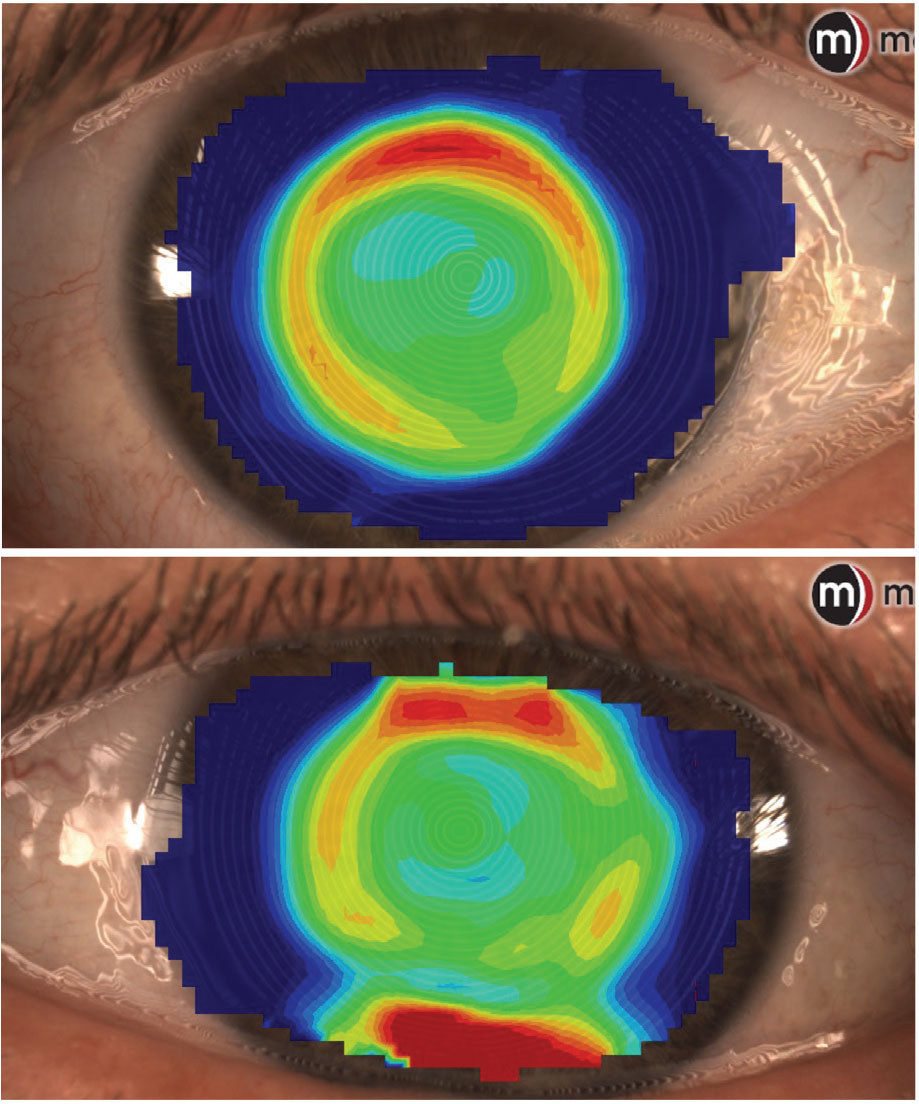
Topography of the right and left eye after skipping ortho-K wear for three nights; note the light but well-centered treatment pattern. Click image to enlarge. |
Discussion
Presbyopia can be a challenging obstacle to conquer when fitting any contact lenses. Focus is typically placed on the best possible distance vision, which can result in a worsening of near vision in many patients with reduced accommodative ability, including those wearing ortho-K. There are many options to address this near demand, including near vision only glasses, refitting into a monovision treatment or using presbyopic ortho-K designs. Patients’ lifestyles will often determine how presbyopia is handled. Are they comfortable wearing reading glasses some of the time? If so, distance vision correction with ortho-K may be ideal. Do they require fine stereopsis or work with sharp detail at near? Monovision may not be the best option for that patient. Ortho-K can be very flexible in the vision it provides patients, and, as a greater number of presbyopic designs are becoming available, it may be a more commonly used presbyopia treatment modality.
Results
This patient requires the ability to see very fine detail at close distances for his typical workday. An extended trial of monovision correction was considered using a soft contact lens to simulate under-correction in the nondominant eye. However, when the patient tried this modality in the office, he immediately noticed that his near vision was reduced, thus prompting him to not elect pursual of monovision.
He was comfortable with his distance vision being slightly blurry, and, as he had reported, he often went multiple nights sleeping without his lenses before returning to them for one to two nights. He felt that this cycle allowed him to maintain very good near vision with usable distance vision most days.
We elected to refract him after a three-night washout period and write a spectacle prescription for distance vision use after not sleeping in his lenses for two to three nights at a time. At his six-month follow-up visit, he reported that his ortho-K cycle was working well, though he was reminded that other modifications will likely be needed as his presbyopia progresses.
Dr. Su is the Cornea and Contact Lens Fellow at the Cornea and Laser Eye Institute (CLEI) Center for Keratoconus. She has no financial interests to disclose.

