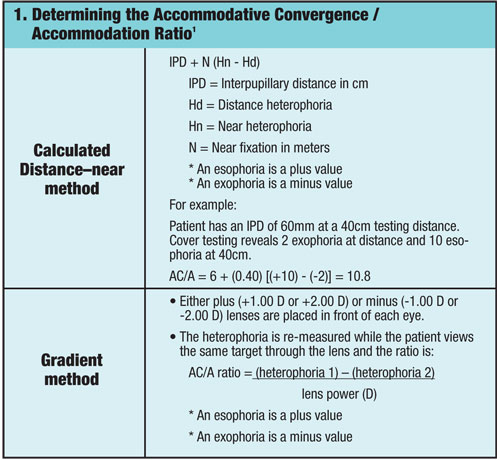
 The use of plus lenses to reduce the demands on the accommodative system is routine in the management of presbyopia. Plus lenses may also be considered in the management for symptomatic relief of intermittent blur, eyestrain and headaches due to an over-taxed accommodative system or for binocular disorders when patients yield a high accommodative convergence to accommodation (AC/A) ratio (figure 1).1 For example, a patient with an AC/A of 10 would increase accommodative convergence by 10r for every 1.00D of accommodation exerted. Thus, small amounts of add power may significantly reduce a patient’s eso-deviation.
The use of plus lenses to reduce the demands on the accommodative system is routine in the management of presbyopia. Plus lenses may also be considered in the management for symptomatic relief of intermittent blur, eyestrain and headaches due to an over-taxed accommodative system or for binocular disorders when patients yield a high accommodative convergence to accommodation (AC/A) ratio (figure 1).1 For example, a patient with an AC/A of 10 would increase accommodative convergence by 10r for every 1.00D of accommodation exerted. Thus, small amounts of add power may significantly reduce a patient’s eso-deviation.
The prescribing of plus lenses requires an understanding of the patient’s visual demands and knowledge of the lens options that fit within the context of those demands. For example, the downward viewing angle required for a bifocal spectacle add power is misaligned to the often straight ahead viewing gaze of a computer. One study found that school children often adopted insufficient downward viewing with a progressive addition lens, reducing its therapeutic effect for near addition.2 Off-axis viewing through a spectacle lens may also induce an unwanted prismatic demand that can exacerbate a binocular disorder. In many cases, pre-presbyopic patients who wear multifocal spectacle lenses are interested in eliminating the use of their spectacles for improved cosmesis and convenience.
Multifocal contact lenses can address the limitations of multifocal spectacle lenses and have been recommended for therapeutic purposes outside of the management of presbyopia.3 Let’s review what is currently known about the effectiveness of commercially available multifocal contact lenses on the management of aphakia/pseudophakia, accommodative dysfunction, binocular disorders and retardation of myopia progression.
Multifocal Contact Lens Design
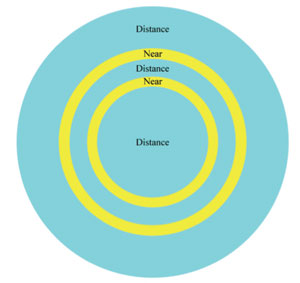
2. A simultaneous bifocal contact lens design includes smaller zones for near vision.
Presently, multifocal contact lenses can be categorized into two lens designs: simultaneous and alternating designs. Simultaneous designs contain regions of the lens designated for near and distant viewing. The distant and near images are viewed simultaneously requiring the patient to discern between the focused and unfocused images (figure 2). Concentric rings and aspheric designs are the two types of simultaneous vision lenses that are presently available in both soft and rigid gas-permeable (RGP) materials. A potential advantage with the aspheric design is an increased depth of focus, providing greater tolerance for small focus errors.4 An alternating design has discrete regions for distant and near viewing that requires a good translation to reach the appropriate focal power (figure 3). This design is most similar to a traditional multifocal spectacle lens and unlike the simultaneous designs, is only available in RGP lenses.
Management of Aphakia and Pseudophakia
Aphakia/pseudophakia is a common indication for medically necessary contact lenses within the pediatric population. In the case of aphakia, silicone elastomer lenses are used because of their power availability (from +7.00D to +35.00D) and high oxygen transmissibility. Following cataract extraction, infants are typically overcorrected by 2.00D to 3.00D to allow for clear retinal images within the infant’s plane of regard.5 As the child develops and becomes aware of more distant objects, the overcorrection is reduced. At approximately two years of age, most aphakic children will undergo intraocular lens (IOL) implantation. Many surgeons select an IOL power to target a resultant refractive error of emmetropia, which over time will require correction of the myopia, as the eye continues to axially elongate.6 A bifocal correction of +3.00D for near is often considered for children with good post-surgical visual acuity and binocular potential.7
An evaluation of various simultaneous (ACC by Salvatori Ophthalmics, Tangent Streak by Fused Kontacts) and alternating (VFL by Conforma Laboratories, and Constavu by Salvatori Ophthalmics) multifocal contact lenses found comfortable wear and acceptable distance and near visual acuity (near acuity >20/30 in at least 67% of patients).8 Limitations of this study were the small sample size of six subjects (Age range: 10-34 years, Mean age: 16 years) and an unrepresentative sample of infantile aphakia with five of the six subjects aphakic due to anterior segment trauma. Presently, the use of multifocal contact lenses in the management of aphakia/pseudophakia has not been extensively reported and studied in the literature.
Management of Accommodative Dysfunction
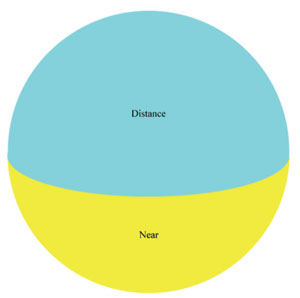
3. An alternating bifocal contact lens design includes a larger near zone on the bottom of the lens.
Patients who have difficulty stimulating and sustaining accommodation have accommodative insufficiency. Diagnostic findings for such patients may include reduced amplitude of accommodation for their age, reduced positive relative accommodation, reduced accommodative facility on the +/-2.00D flipper test, and/or demonstrate a lag of accommodation on monocular estimated method (MEM). In the absence of a large heterophoria, prescribing near addition lenses for patients with accommodative insufficiency serves to reduce asthenopic symptoms associated with exerting sufficient accommodation to meet the accommodative demand.1 The amount to prescribe at near is often determined by the lens power necessary to normalize accommodative findings such as MEM or by balancing the NRA and PRA findings.
In theory, a multifocal contact lens should be an equivalent management option to multifocal spectacle lenses. One case report describes the use of multifocal contact lenses in the management of a symptomatic 23-year-old patient who was diagnosed with accommodative insufficiency.9 The patient was prescribed a bifocal contact lens with a +1.25D add and reported immediate comfort and increased clarity while reading. Studies specifically looking at the use of multifocal contact lenses in the management of accommodative dysfunction have not been published; however, it is regarded as an alternative to multifocal spectacle lenses.3
Management of Convergence Excess and Accommodative Esotropia
Convergence excess and accommodative esotropia are binocular conditions associated with a high AC/A ratio. Convergence excess presents with an eso-deviation that is greater at near, and accommodative esotropia with an esotropia at near.10 Early detection and appropriate refractive management are especially important in cases of accommodative esotropia to ensure good visual acuity, ocular alignment and sensory fusion.11
Appropriate management often includes a cycloplegic refraction where the full hyperopic refractive error is corrected and possibly near addition lenses if a residual eso-deviation is observed at near.12-14 The power of the addition lens is typically the least amount of plus that reduces the eso-deviation in cases of convergence excess and to establish binocular alignment in patients with accommodative esotropia. Long-term follow-up studies have found that children who require the use of multifocal spectacles to maintain binocular alignment continue to need them through adolescence and adulthood.15-17
 Although multifocal spectacle lenses have been successful in the control of eso-deviations at near, reports using multifocal contact lenses have not shown the same success. In one case report, simultaneous aspheric RGP multifocal contact lenses were used in the management of a patient with convergence excess.18 In comparing +1.50D bifocal spectacle lenses to aspheric multifocal contact lenses, spectacles reduced the esophoria at near from 8∆ esophoria at near to 1∆ esophoria and the multifocal contact lenses reduced the phoria to 3∆ esophoria. Although better results were attained with spectacles, the patient continued with lens wear because of symptomatic relief and improved cosmesis.
Although multifocal spectacle lenses have been successful in the control of eso-deviations at near, reports using multifocal contact lenses have not shown the same success. In one case report, simultaneous aspheric RGP multifocal contact lenses were used in the management of a patient with convergence excess.18 In comparing +1.50D bifocal spectacle lenses to aspheric multifocal contact lenses, spectacles reduced the esophoria at near from 8∆ esophoria at near to 1∆ esophoria and the multifocal contact lenses reduced the phoria to 3∆ esophoria. Although better results were attained with spectacles, the patient continued with lens wear because of symptomatic relief and improved cosmesis.
Another study compared the effectiveness of two different simultaneous aspheric design contact lenses, Frequency 55 Multifocal (CooperVision) and Unilens 38 Multifocal (Unilens), to bifocal spectacle lenses in a patient with accommodative esotropia.19 The bifocal spectacle lenses were able to correct the strabismus, but neither contact lens resulted in acceptable binocular alignment and stability. Another study was terminated prematurely due to disappointing results with two simultaneous design lenses, SimulVue Bifocal (Unilens) and Unilens Aspheric RGP (Unilens).20 Five of the six patients were found to have eso-deviations at near through the contact lenses as large as that found when looking through the distance portion of their spectacles.
The alternating design of Tangent Streak bifocal contact lenses (Fused Kontacts) was used in the management of three patients with accommodative esotropia.21 The authors reported that motility and stereo acuity measurements in patients wearing bifocal contact lenses were similar to the measurements of those wearing bifocal spectacle lenses. They concluded that the Tangent Streak lens was an acceptable alternative to bifocal spectacles. However, two of the three patients manifested a constant esotropia at near through the Tangent Streak contact lenses that was not present through bifocal spectacles.
Studies showing the effectiveness of using multifocal contact lenses in the management of patients with convergence excess and accommodative esotropia are limited. Most of the studies utilized simultaneous vision multifocals, and one author postulated that, unlike presbyopic patients, younger children may have sufficient accommodation to choose the image that requires more effort, thereby negating the plus effect.4 Based on these early reports, multifocal spectacle lenses continue to be a better refractive management option for those with convergence excess and accommodative esotropia.
Myopia Control
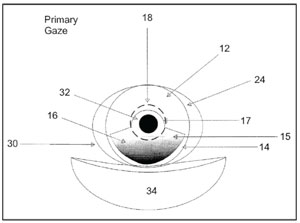
5. United States Patent 7559650, manufacturing techniques for the production of hydrodynamic multifocal contact lenses.30
The described lens design is a soft contact lens that would dynamically
alter the optical power through gaze dependent fluid dynamics.
Anecdotal studies of RGP lenses have led clinicians to utilize them as a method to stop myopic progression. Only recently have the rigors of a randomized clinical trials concluded that RGP lenses do not slow the progression of myopia.22 Prospective case series on corneal reshaping lenses by the Longitudinal Orthokeratology Research in Children (LORIC) and Corneal Reshaping and Yearly Observation of Myopia (CRAYON) study groups have suggested an effect on slowing axial elongation, but there have been no randomized clinical trials to validate this finding.23, 24
Multifocal spectacle lenses have also been prescribed for the retardation of myopia based on the theory that retinal defocus experienced when insufficient accommodation is exerted during nearwork causes axial elongation.25,26 This theory was somewhat supported by the results of Correction of Myopia Evaluation Trial (COMET), where myopic children with accommodative lag (≥0.43D for a 33cm target) and near esophoria benefited from reduced progression of myopia with a +2.00D progressive addition lens vs. single-vision lenses.
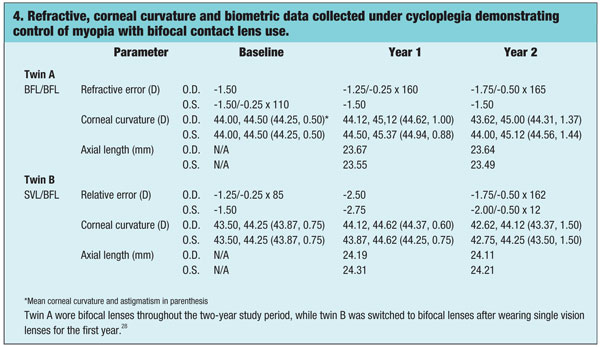
An improved treatment effect with multifocal contact lenses vs. multifocal spectacles has been demonstrated in the literature.27 Children younger than 16 years of age who previously wore multifocal spectacles but were still progressing in their myopia were subsequently treated with soft multifocal contact lenses with a simultaneous design. After 12 months of using the multifocal contact lenses, 24 subjects progressed a mean of -0.18 ± 0.23D (p<0.001), and 12 subjects showed no significant progression. This was compared to the previous progression rate with multifocal spectacles of -0.56 ± 0.17D per year. The use of multifocal contact lenses to correct retinal defocus was also the premise in a case report of 12-year-old identical twin girls with low baseline myopia and associated eso-deviation at near.28 Twin A was prescribed a simultaneous concentric design bifocal contact lens, and Twin B was prescribed a single-vision contact lens. A +2.00D add was used based on the least amount of add power to neutralize the near fixation disparity. In contrast to Twin B, Twin A demonstrated minimal progression during the first 12 months; Twin B experienced the same stabilization following the crossover at 12 months (figure 4).
Although preliminary studies suggested a cessation of myopia progression with multifocal contact lens use, the theorized effect of improved accommodative accuracy was not evidenced.29 The authors of the twin study theorized that the use of multifocal contact lenses may slow the progression of myopia simply through improved compliance of the add power, as dependency on appropriate gaze was no longer an issue.2,28 The effectiveness of multifocal contact lenses as a control for myopia progression remains speculative until a randomized clinical trial has been reported.
Follow Up to Ensure Success
As an off-label management consideration, results of presently available multifocal contact lenses have been mixed with little evidence to supports its use. This may be due to the inability of multifocal contact lenses to effectively provide a single yet dynamic focal power that is appropriate to the prescribed indication. United States Patent 7559650, issued on July 14, 2009, described a novel contact lens manufacturing technique, where the lens would mimic the ability of the human lens to dynamically change focus.30 The ability for the contact lens to change its refractive power would be through a reservoir of fluid that can dynamically shift from the periphery to the center based on the pressure exerted by the eyelids in different fields of gaze (figure 5). Until such a lens becomes available, a practitioner may still consider using presently available multifocal contact lenses as an off-label management to spectacles. But remember: appropriate follow-up steps should be taken to ensure that the desired improvement of the patient’s symptoms and/or findings is achieved.
1. Cooper J, Burns C, Cotter S, et al. Care of the patient with accommodative and vergence dysfunction. American Optometric Association. 1998.
2. Hasebe S, Nakatsuka C, Hamasaki I, Ohtsuki H. Downward deviation of progressive addition lenses in a myopia control trial. Oph Phys Optics. 2005 Jul;25(4):310-4.
3. Weissman B, Barr J, Harris M, et al. Care of the Contact Lens Patient. 2nd ed. St. Louis, MO: American Optometric Association. 2006.
4. Moore B. Pediatric contact lenses: case reports. J Am Optom Assoc. 1998 Feb;69(2):88-114.
5. Hom M, Bruce A. Manual of Contact Lens Prescribing and Fitting with CD-ROM. 3rd ed. St. Louis, Mo. Butterworth-Heinemann; 2006.
6. Wilson M, Trivedi R, Pandey S. Pediatric Cataract Surgery: Techniques, Complications, and Management. Philadelphia. Lippincott Williams & Wilkins. 2005.
7. Hayashi K, Hayashi H. Stereopsis in bilaterally pseudophakic patients. J Cataract Refract Surg. 2004 Jul;30(7):1466-70.
8. Conklin JD, Litteral G, Schmeisser ET, Van Meter WS. An evaluation of four multifocal contact lenses in young monocular aphakic patients. CLAO J. 1992 Apr;18(2):92-4.
9. Rodgin S. Creative cures using contact lenses. Available at: www.clspectrum.com/article.aspx?article=102552. (Accessed December 2009).
10. Duane A. A new classification of the motor anomalies of the eyes based upon physiological principles. Ann Ophthalmol Otolaryngol. 1897;6:84.
11. Caloroso E, Rouse M. Clinical Management of Strabismus. Boston. Butterworth-Heinemann. 1993.
12. Cotter SA, Edwards AR, Wallace DK, et al. Treatment of anisometropic amblyopia in children with refractive correction. Ophthalmology. 2006 Jun;113(6):895-903.
13. Scheiman M, Wick B. Clinical Management of Binocular Vision: Heterophoric, Accommodative, and Eye Movement Disorders. 3rd ed. Philadelphia. Wolters Kluwer Health/Lippincott Williams & Wilkins. 2008.
14. Javal E. Manuel Theorique et Pratique du Strabisme. Paris: Masson;1896.
15. Swan KC. Accommodative esotropia long range follow-up. Ophthalmology. 1983 Oct;90(10):1141-5.
16. Rutstein RP, Marsh-Tootle W. Clinical course of accommodative esotropia. Optom Vis Sci. 1998 Feb;75(2):97-10.
17. Kubota N, Akatsu S. Long-term follow-up of refractive accommodative esotropia. In: Campos EC, ed. Strabismus and Ocular Motility Disorders: Proceedings of the Sixth Meeting of the International Strabismological Association. Basingstoke Hampshire. Macmillan Press.1991:315-18.
18. Winkler TD. Aspheric contact lenses used to control convergence excess. Clin Exp Optom. 1993 Apr;76(4):141-2.
19. Gonzalez E, Barra F, Sanchez I, et al. High AC/A accommodative esotropia strabismus treated with contact lenses: a single case design (N=1) study. Binocul Vis Strabismus Q. 2007;22(2):90-5.
20. Morton GV, Kushner BJ, Lucchese NJ, et al. The efficacy of SimulVue and Unilens RGP aspheric bifocal contact lenses in the treatment of esotropia associated with a high accommodative convergence/accommodation ratio. J AAPOS. 1998 Apr;2(2):108-12.
21. Rich LS, Glusman M. Tangent Streak RGP bifocal contact lenses in the treatment of accommodative esotropia with high AC/A ratio. CLAO J. 1992 Jan;18(1):56-8.
22. Walline JJ, Jones LA, Mutti DO, Zadnik K. A randomized trial of the effects of rigid contact lenses on myopia progression. Arch Ophthalmol. 2004 Dec;122(12):1760-6.
23. Cho P, Cheung SW, Edwards M. The longitudinal orthokeratology research in children (LORIC) in Hong Kong: a pilot study on refractive changes and myopic control. Curr Eye Res. 2005 Jan;30(1):71-8.
24. Walline JJ, Jones LA, Sinnott LT. Corneal reshaping and myopia progression. Br J Ophthalmol. 2009 Sep;93(9):1181-5.
25. Smith EL, Hung LF, Harwerth RS. Effects of optically induced blur on the refractive status of young monkeys. Vision Res. 1994 Feb;34(3):293-301.
26. Gwiazda J, Thorn F, Bauer J, Held R. Myopic children show insufficient accommodative response to blur. Invest Ophthalmol Vis Sci. 1993 Mar;34(3):690-4.
27. McBrien NA, Morgan IG. Myopia: Proceedings of the 12th International Conference. Optom Vis Sci. 2009;86(1):E67-E73.
28. Aller TA, Wildsoet C. Bifocal soft contact lenses as a possible myopia control treatment: a case report involving identical twins. Clin Exp Optom. 2008 Jul;91(4):394-9.
29. Tarrant J, Severson H, Wildsoet CF. Accommodation in emmetropic and myopic young adults wearing bifocal soft contact lenses. Ophthalmic Physiol Opt. 2008 Jan;28(1):62-72.
30. Iuliano M. Manufacturing techniques for the production of hydrodynamic multifocal contact lenses. 2009. Available at: www.freepatentsonline.com/7559650.html. (Accessed December 2009).

