 |
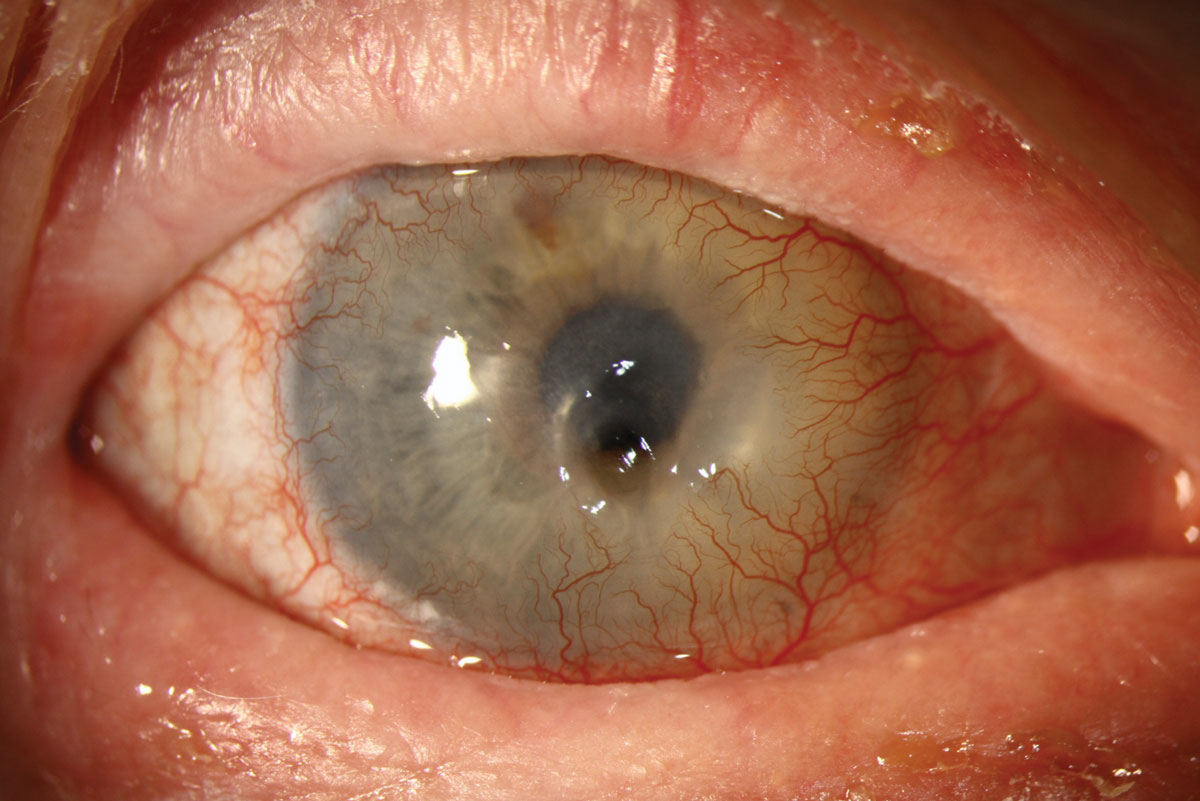
A 66-year-old white male sustained a job-related alkaline burn to his right eye 23 years prior to presentation at the clinic. The cornea referral note indicated advanced limbal stem cell dysfunction, with a completely opaque and vascularized cornea. He was experiencing increasing discomfort and was referred for a possible bandage or scleral contact lens fit to relieve pain.
Upon examination, I noted a central clear area with a scant 30µm of corneal tissue in the 2x2mm clear zone. He was diagnosed with a descemetocele, immediately glued with tissue adhesive and administered a soft bandage lens. He was given topical and oral antibiotics as prophylaxis in case of perforation before he could return. An emergent mini-tectonic penetrating keratoplasty (PKP) surgery was performed at the soonest available time.
A descemetocele is a focal area of corneal thinning in which only Descemet’s membrane remains. There will appear to be a clear, non-vascularized bulge of Descemet’s through the overlying stroma and epithelium. Fluorescein will stain the area; it should be used to look for a positive Seidel sign, since this condition will lead to perforation.
Descemetoceles may form in an eye with a history of infection of any etiology but particularly herpes virus. Other common causes include corneal trauma, chemical injury, exposure keratitis, severe dry eye conditions (e.g., Stevens-Johnson syndrome, Sjögren’s syndrome, vitamin A deficiency, graft-vs.-host disease), post ocular surgery, continuous wear contact lenses and underlying autoimmune diseases. A descemetocele may spontaneously form days, months, years or even decades after the original ocular insult.
Treatment includes lubrication, oral vitamin C to stimulate collagen production, antibiotics to prevent or treat infection, steroid drops if there is concomitant inflammation, oral tetracycline for its anti-collagenase properties, topical cyclosporine, an immunosuppressive, tissue adhesives (cyanoacrylate or autologous human fibrin glue), amniotic membrane transplantation and, ultimately, PKP or a conjunctival flap.
Prognosis for descemetocele is guarded, and the patient should be counseled on the likelihood of a poor visual outcome.
 |
| Click image to enlarge. |

