  |
Gone are the days of reading glasses as your first, last and only option for presbyopia. Whether your scleral lens patient has a regular or irregular cornea, you can present the option of multifocal optics more confidently than ever before. Laboratories are offering simultaneous multifocal optics in their scleral designs, and the ability to customize them contributes to their success. Today, you can change add power or zone size and decenter the optics in the lens. A methodical approach to patient education and fitting can improve your success when offering these lenses to patients.
Manage Expectations
With multifocal lenses, the visual outcome can hinge on a patient’s expectations of what is considered successful completion of the fit. A patient’s visual demands are going to largely determine their definition of success. Before you offer a multifocal to your scleral lens patient, a detailed case history will allow you to determine their near vision demands, daily tasks and work environment. Also, gauge their potential for dissatisfaction with less than perfect vision based on their personality and lens wear history.
For regular cornea patients who demand the highest quality vision, consider whether a translating gas permeable (GP) lens may be an option instead of a scleral lens. Simultaneous vision optics are really the only option with scleral and hybrid lenses because the lenses do not move or translate on-eye.1 While this effect can contribute to stability, the optics must be centered properly over the visual axis for success. In irregular cornea patients who have reduced distance acuity, wearing glasses over their contact lenses may provide the best near vision.
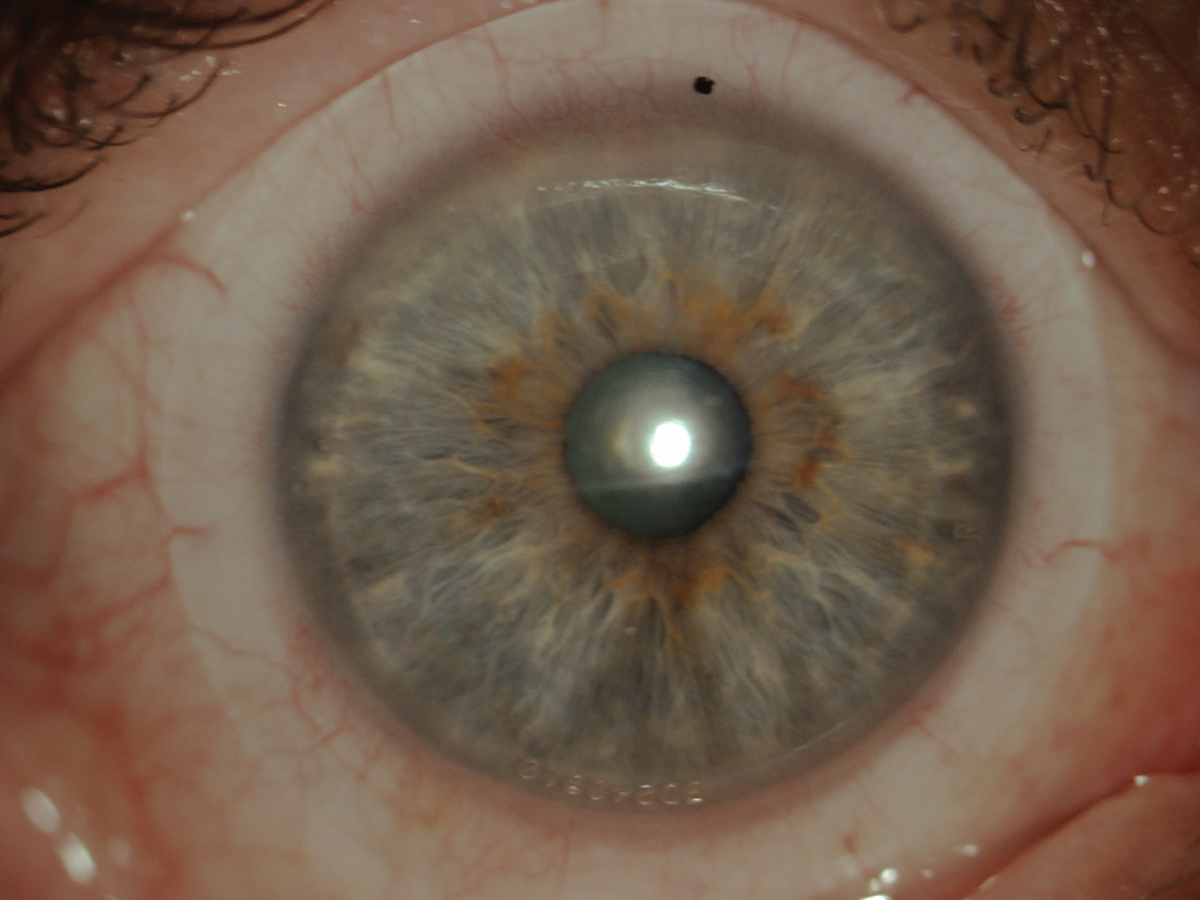 |
| This multifocal scleral was ordered after the single vision lens was fit successfully and best distance acuity achieved. Click image to enlarge. |
The cost of a multifocal scleral may also be a deciding factor for some patients. Educate them that the cost may be similar to a daily disposable soft multifocal lens. For patients who are not willing to make the investment, you can consider a monovision or modified monovision scleral lens option or a monthly/biweekly multifocal soft contact lens. Demonstrating the monovision experience in-office can be useful for these patients. Keep in mind that patients may still need to supplement with reading glasses, so discuss this possibility upfront to reduce disappointment later.
Manufacturers recommend achieving a satisfactory fit (central clearance, limbal vault, edge alignment, patient vision and comfort) with a single-vision product and having successful follow-up prior to adding multifocal optics. This can take up to four or more visits, depending on the cornea, the complexity of the fit and the experience of the fitter.2 The addition of multifocal optics to the lens design may add another visit or two to achieve success.
Special Features
When fitting multifocal sclerals, focus on two features:
Decentered optics. Large-diameter scleral lenses often decenter and can present a challenge to the practitioner. Lenses with excessive central vault also tend to decenter.3
One study showed that it is more common for a lens to decenter than to properly center.4 The lens tends to follow the contours of the sclera, positioning in the opposite direction of the patient’s line of sight. Adding simultaneous vision optics in a decentered lens can cause issues with distance acuity, near acuity or both. Studies suggest visual improvement when soft lens optics are decentered (and over the line of sight), and that improvement is the impetus for decentered optics in scleral designs.5,6 Some fitting sets include lens markings that help determine the appropriate angle and offset amount for the near zone, while other sets use a standard design you can modify.
Variable zones. Consider whether changes to the near zone size can improve your results with multifocal lenses. Most designs on the market today have a center-near zone. Assess the patient’s pupil size, as a smaller pupil may experience difficulties in bright light since more of the near zone is being viewed through the pupil. A larger pupil may have difficulty using the near zone at all if the pupil does not constrict enough or the light is dim. The multiple zones of scleral lens power require the proper alignment to deliver light to the retina and provide good near, intermediate and distance vision simultaneously. Having a variable near zone option allows for more flexibility to reach the patient’s visual goals if the acuity is at a suboptimal level despite proper lens centration.
Case One
A 67-year-old Caucasian male presented with complaints of discomfort and blur at near with his habitual multifocal hybrid lenses. As a longstanding patient, we were aware of his Type A personality and particular visual demands. We spent extensive time detailing realistic expectations with multifocal lenses, including a range of refit options—modifying the current hybrid lens design, switching to a GP design or attempting a scleral multifocal design. The patient insisted on trying the multifocal scleral. So, he was fit in a Zen RC (Bausch + Lomb) initially with the later addition of multifocal optics (Zen Multifocal) after the single vision lens was fit successfully and best distance acuity achieved.
We reduced the add and included a smaller near zone to the design of the Zen RC for the dominant eye. The axis was shifted OU to account for lens rotation, and the final lens allowed the patient to achieve 20/20 vision OU at near. Adding Hydra-PEG (Tangible Science) to each lens ensured optimal comfort, given the entering complaint of discomfort with his habitual hybrid lenses.
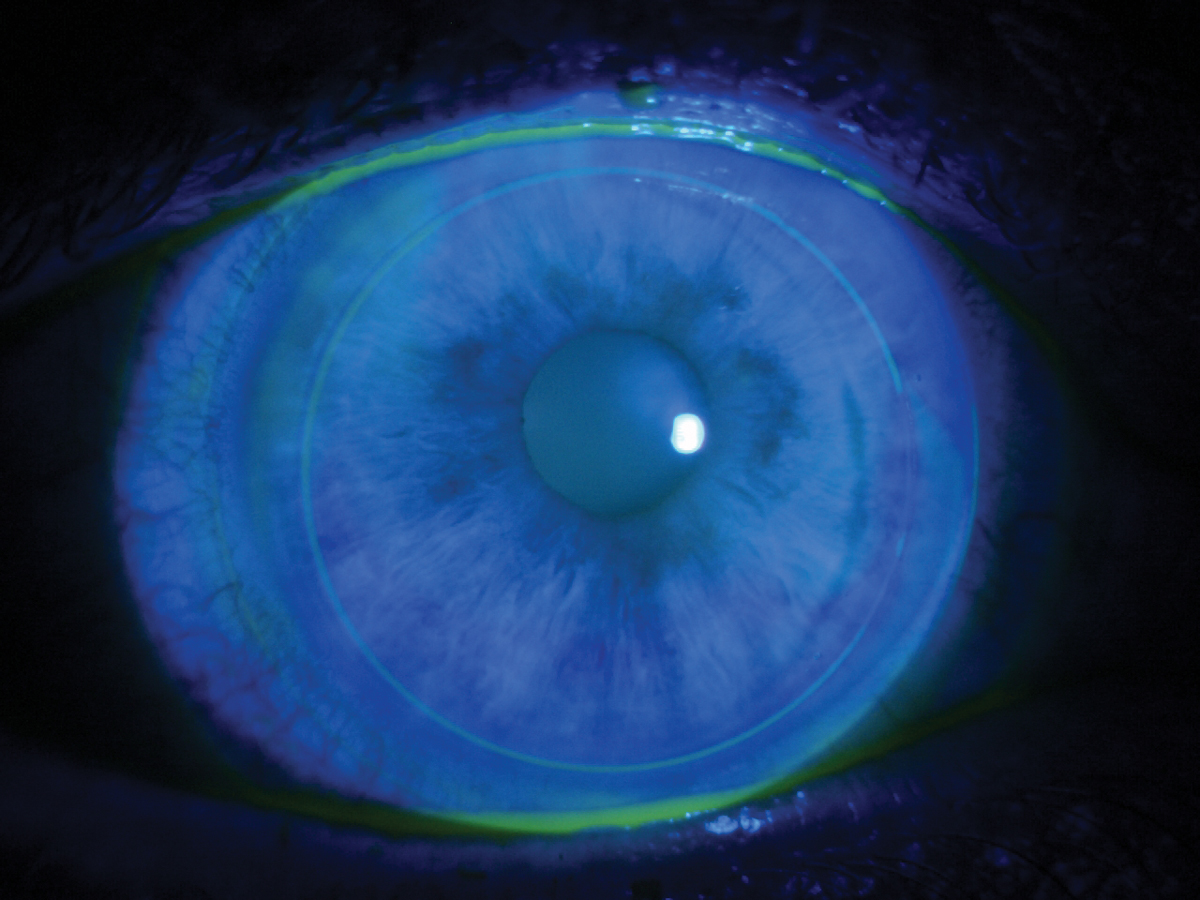 |
| Markings on some scleral lens fitting sets can assist you in evaluating lens zones and centration. Click image to enlarge. |
A 47-year-old Caucasian female presented complaining of blur, haloes and photophobia OS related to corneal scarring secondary to herpes zoster viral infection. She had been wearing multifocal soft lenses for the last three years with a best-corrected visual acuity of 20/20 OD, 20/30 OS and J3 OU at near. The patient was refit into a Zen Multifocal OS while continuing wear of the soft multifocal lens OD. Upon dispense of her new lens OS, vision was 20/20 OD, 20/25 OS and J2 OU at near. She was satisfied with her overall vision improvement at both distance and near but still wished to have sharper distance vision OS.
In cases of a distance vision complaint, the laboratory recommends removal of the near zone decentration option. Theoretically, this should sharpen the distance vision without a substantial loss in near acuity, as the near optics are no longer in the patient’s visual axis. With this small adjustment incorporated, the patient was thrilled with both her distance and near vision.
There are several different ways to approach troubleshooting when a distance or near complaint exists with a multifocal scleral lens. Much of your decision-making will depend on the lens design and the fitting guide. A quick call to the laboratory consultation department can also point you in the right direction. We find it especially useful in tough cases to consider lens designs that have special features such as decentered optics and/or custom near zone sizes. Your presbyopic patients often have the disposable income to invest in these technologies, and they will surely appreciate your dedication to their visual needs.
| 1. van der Worp E, Bornman D, Ferreira DL, et al. Modern scleral contact lenses: a review. Cont Lens Anterior Eye. 2014;37(4):240-50. 2. Macedo-de-Araújo RJ, van der Worp E, & González-Méijome JM. Practitioner learning curve in fitting scleral lenses in irregular and regular corneas using a fitting trial. BioMed Res Int. 2019.2019;1-11. 3. van der Worp E. A Guide to Scleral Lens Fitting, Version 2.0. Forest Grove, OR: Pacific University; 2015. Available: commons.pacificu.edu/mono/10/. Accessed February 5, 2020. 4. Ramdass S, Rosen C, Norman C, Buckingham R. Clinical analysis of scleral lenses on regular corneas. Presentation at: Global Specialty Lens Symposium. Las Vegas, NV. January 2016. 5. Brujic M. The importance of optical placement in multifocal lenses. Presentation at: Global Specialty Lens Symposium. Las Vegas, NV. January 2015. 6. Zheng F, Caroline P, Lampa M, et al. Visual effects of centered and decentered multifocal optics. Poster presented at the Global Specialty Lens Symposium, January 2016, Las Vegas. |

