 |
This patient presented with a left-eye history of posterior capsule rupture during initial cataract extraction, with subsequent posterior dislocation of the intraocular lens. The subluxed lens was retrieved and a scleral-fixated intraocular lens (IOL) was attempted, which too fell posteriorly. This resulted in a shallow temporal retinal detachment. He was seen by a retina surgeon, who performed pars plana vitrectomy for removal of remaining capsular material, as well as laser repair of the temporal rhegmatogenous retinal detachment. A sutureless scleral-fixated IOL was applied at this time.
Around three weeks post-IOL placement, the patient noted a decline in vision and was found to have a recurrent rhegmatogenous retinal detachment, for which he underwent pars plana vitrectomy for exploration and repair.
Following the final RD repair surgery, the left eye had persistent ocular hypertension, raising concern for progressive pupillary block/synechiae formation. He was managed on timolol-dorzolamide (Cosopt) and Diamox, and underwent a YAG laser iridotomy. Despite this, the intraocular pressure remain elevated (in the low-30s) with shallow chamber due to the gas bubble (needed for the retinal detachment repair) and limited adherence to positioning (per family’s report).
 |
|
Click image to enlarge. |
He was taken back to the operating room for synechiolysis and deepening of the chamber, to resolve the pupillary block. Intraoperatively, he was found to have 360° iris and corneal synechiae and occluded angle. After lysis of these synechiae, he had blood staining of the central cornea. The staining and endothelial failure required Descemet’s membrane endothelial keratoplasty (DMEK) and subsequent rebubble.
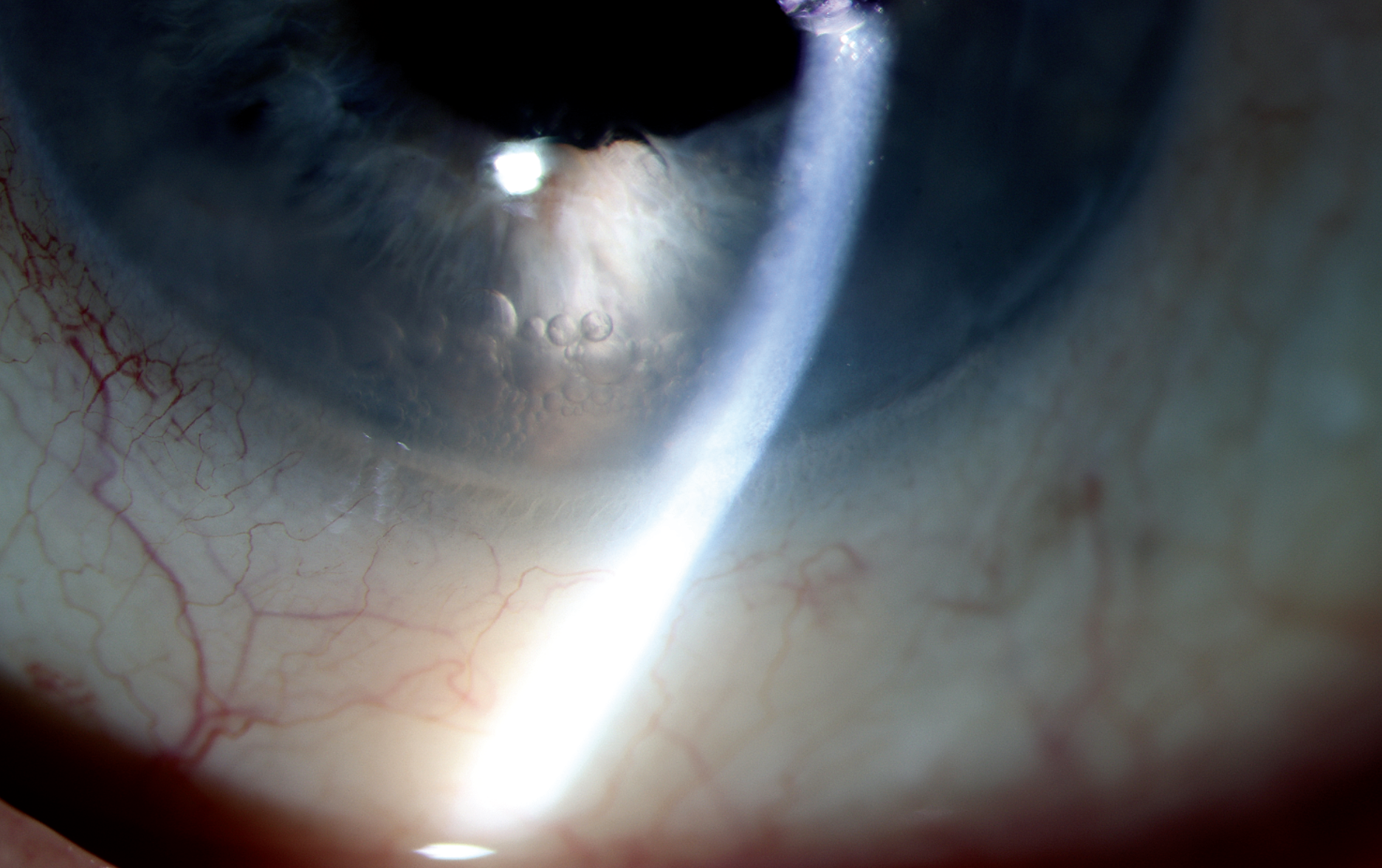
In this photo, accumulation of small perfluorocarbon bubbles in the anterior chamber is observed. His entering visual acuity is 20/60, with an IOP of 8mm Hg. The DMEK tissue is well attached and the cornea is clear and compact. Mild cystoid macular edema was found on examination. He is being maintained on prednisolone acetate QID and Cosopt BID.

