 |
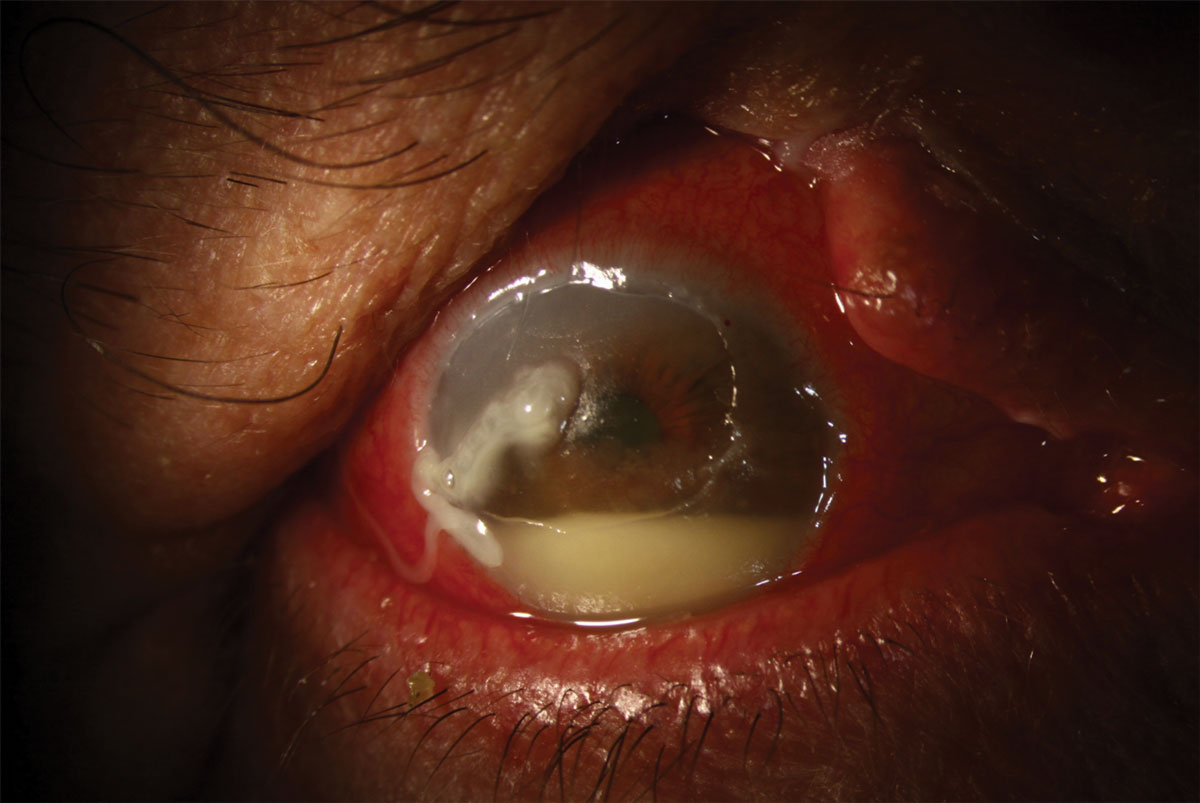
A 72-year-old male presented with a history of excision of squamous cell carcinoma of the right upper lid one month prior. His post--op course has been complicated by wound dehiscence and subsequent exposure keratopathy. On exam, he had >80% of the upper lid missing along with brow ptosis with trichiasis, dermatochalasis and a >60% lagophthalmos. The conjunctiva had 4+ injection with mucous discharge. The cornea had a large central/superior epithelial defect with rolled edges and stromal thinning. No infiltrate was present, but there was a 3.5mm hypopyon.
 |
|
Click image to enlarge. |
His history and exam are concerning for a sterile corneal melt in the setting of exposure keratopathy and possible HSV keratouveitis. An amniotic membrane was placed and fortified vancomycin and fortified tobramycin were started Q2h, along with artificial tear ointment. He was instructed to start doxycycline 100mg BID, vitamin C 1000mg BID and valacyclovir 1,000mg TID.
Exposure of the ocular surface has led to corneal anesthesia, known as neurotrophic keratopathy (NK). Loss of corneal sensation leads to progressive morphological and metabolic epithelial abnormalities and the development of epithelial defects and ulcers. When the underlying stroma is exposed, melting and progression to corneal perforation is possible.
NK is classified into three stages—(1) corneal epithelial changes, (2) persistent epithelial defects and (3) corneal ulceration with stromal involvement—and this staging guides treatment goals. Stage 1: prevent epithelial breakdown. Stage 2: prevent infection and mechanical epithelial disruption. Stage 3: intervene surgically to protect against perforation.
The hypopyon in this case is a collection of cells (leukocytes, erythrocytes and macrophages), fibrin and proteins and reflects the severe inflammatory status of this patient. The herpes virus should always be considered as a confounding factor in cases of NK and severe ocular inflammation. NK should always be considered in cases where signs outweigh patient symptoms.
This case is complicated by the patient’s relative lack of compliance and heavy smoking habit. The very high risk of permanent vision loss or loss of the eye was emphasized to this patient. While lid reconstruction is the ultimate goal, ocular surface protection with a scleral lens is the first long-term treatment plan.

