 |
When fitting a GP lens on a patient with any prior history of ocular surgery, it is crucial to perform a complete anterior segment evaluation. This will allow you to clearly see any “obstacles” to the fitting process and select an appropriate lens modality. Depending on the patient’s history, these obstacles could be pingueculae, sutures, a filtering bleb, a tube shunt or some combination of the aforementioned. While corneal GP lenses may seem to be an ideal option for these patients, the fits can be challenging, and close follow-up is warranted. The overall diameter of the corneal lens should be altered to avoid or vault any associated obstacles. It is crucial to remove the lens and stain the cornea at each follow-up visit to ensure there are no adverse effects on the ocular surface (or the ocular obstacles).
Case #1
A 62-year-old habitual ThinSite (Art Optical) corneal GP lens wearer with degenerative myopia and primary open-angle glaucoma OU presented for a re-fit after complicated cataract extraction with MIGS OU. The corneal GP parameters prior to surgery were OD 7.5/9.5/-24.25DS with a BCVA of 20/200 and OS 7.50/9.5/-26.50DS with a BCVA of 20/80+. Visual acuity was more limited OD due to prior retinal detachment and subsequent repair two years prior. Externals were notable for a 2+ APD OD and a constricted visual field by confrontation OD.
 |
|
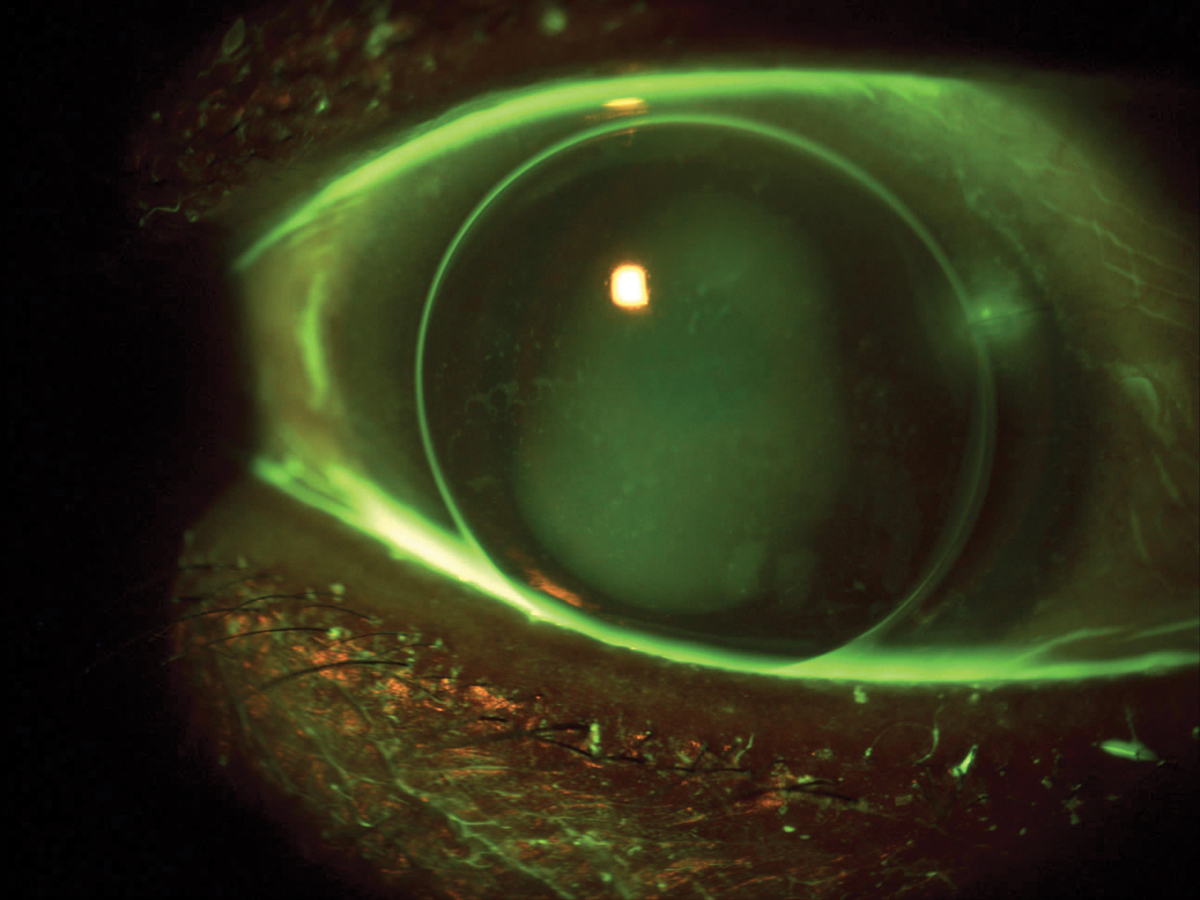
Fig. 1. Corneal lens on eye with nasal embedded corneal suture showing staining. Overall fit was steep, so the lens was reordered with a smaller diameter to improve fit and avoid the suture. Click image to enlarge. |
Anterior segment findings included a filtering bleb with tube shunt superior temporal OD along with residual embedded sutures both nasal (one) and inferior temporal (two). The patient is pseudophakic OU. We fit in ThinSite corneal lenses with parameters OD 7.30/9.0/-10.50DS and OS 7.20/9.0/-5.00DS based on fit and over-refraction of her habitual lenses, bringing her vision to 20/80 OD, 20/50+ OS, and 20/40- OU. The lenses were dispensed.
The patient returned for follow-up one month later reporting that the lens material was “too soft” and that she “could not hear the lenses when she dropped them” as she could in the past. While the lenses were manufactured in the same Boston EO material worn previously, we suspect she was noticing the thinner edges of the now lower-powered lens. Despite this issue, she thought the lenses were comfortable overall, and noted her vision was stable. Slit lamp exam revealed corneal fluorescein staining in an area surrounding the suture at two o’clock OS (Figure 1). The patient was advised to limit wear time, use preservative-free artificial tears every hour to lubricate the eye, and the lens was reordered in a smaller overall diameter OS (Figure 2).
The new 7.20/8.5/-4.50DS lens allowed the lens edge to land further inward from the embedded sutures. After dispense, she returned for follow-up several weeks later to reveal no staining in the area of concern. Given the reduced best-corrected vision in corneal lenses, we prescribed bifocal glasses for full-time wear over the top in polycarbonate material.
Case #2
A 30-year-old female with history of trauma to the left eye in 2023 with surgical repair and resultant aphakia presented for a first-time contact lens fitting in the left eye only. Entering uncorrected visual acuity was 20/20 OD, 20/200 (pinhole 20/100) OS. Externals were notable for an irregular superonasally displaced pupil OS.
 |
|
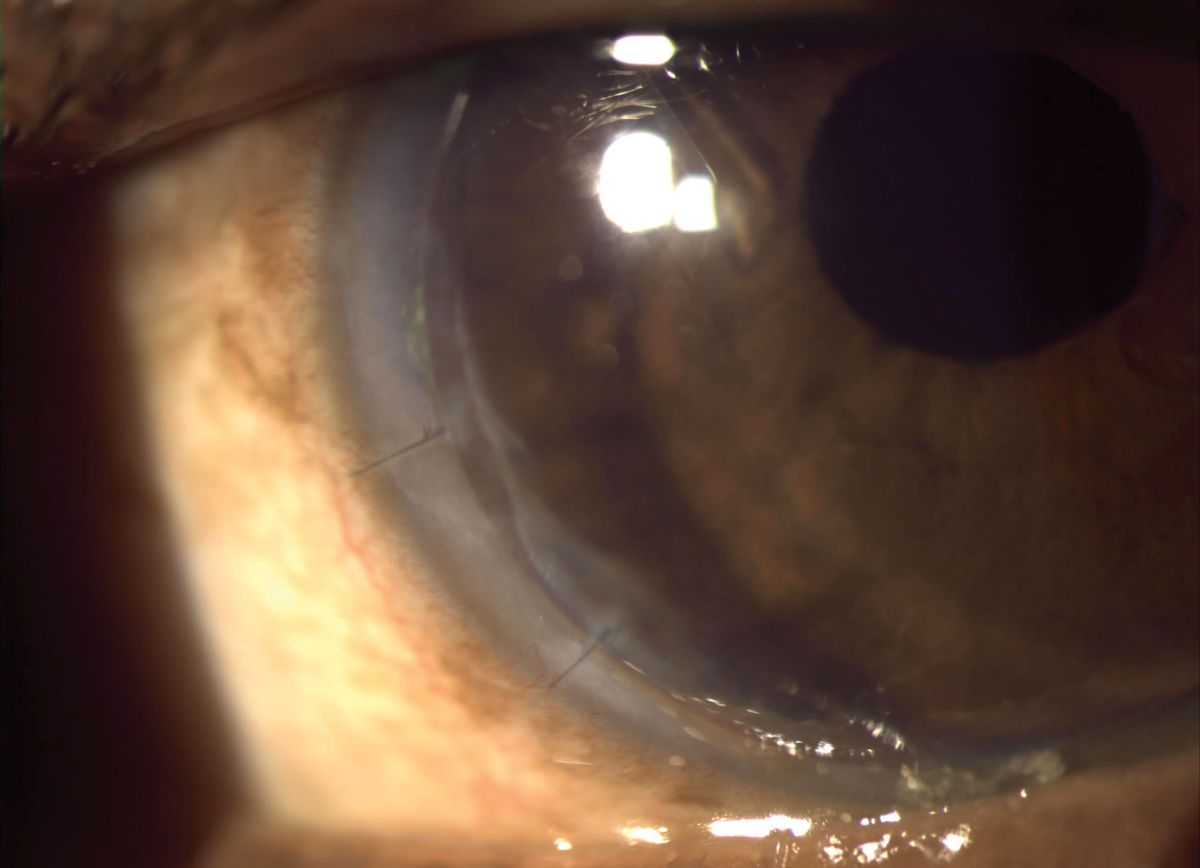
Fig. 2. The smaller overall diameter also helped avoid staining at the inferotemporal embedded sutures in Case #1. Click image to enlarge. |
Refraction was OD +0.25DS with BCVA 20/20 and OS +13.00 -2.00x036 with BCVA of 20/25. Anterior segment findings were unremarkable OD. Findings OS included two sutures superonasal located temporal to the limbus, an irregular pupil margin decentered superonasal and iridodonesis.
The patient was fit diagnostically with a Biofinity XR Toric soft contact lens (CooperVision) achieving 20/20 vision, but there was some concern as the lens edge landed near the existing conjunctival sutures. A ThinSite corneal lens was trialed OS with BCVA 20/20. The patient proceeded with the GP lens due to reduced risk of complications as the sutures could be avoided. The initial order was for ThinSite +15.75/7.6/9.50/Boston EO (Art Optical) OS only.
At the initial dispensing visit, the patient was able to see 20/20 OS with a plano over-refraction. Evaluation revealed that the lens was decentered inferotemporally. While this was ideal as it avoided the two sutures superonasal, the pupil was not fully covered due to its superonasal displacement. The lens was reordered with a 10.0mm diameter to increase the sagittal height and improve centration.
 |
|
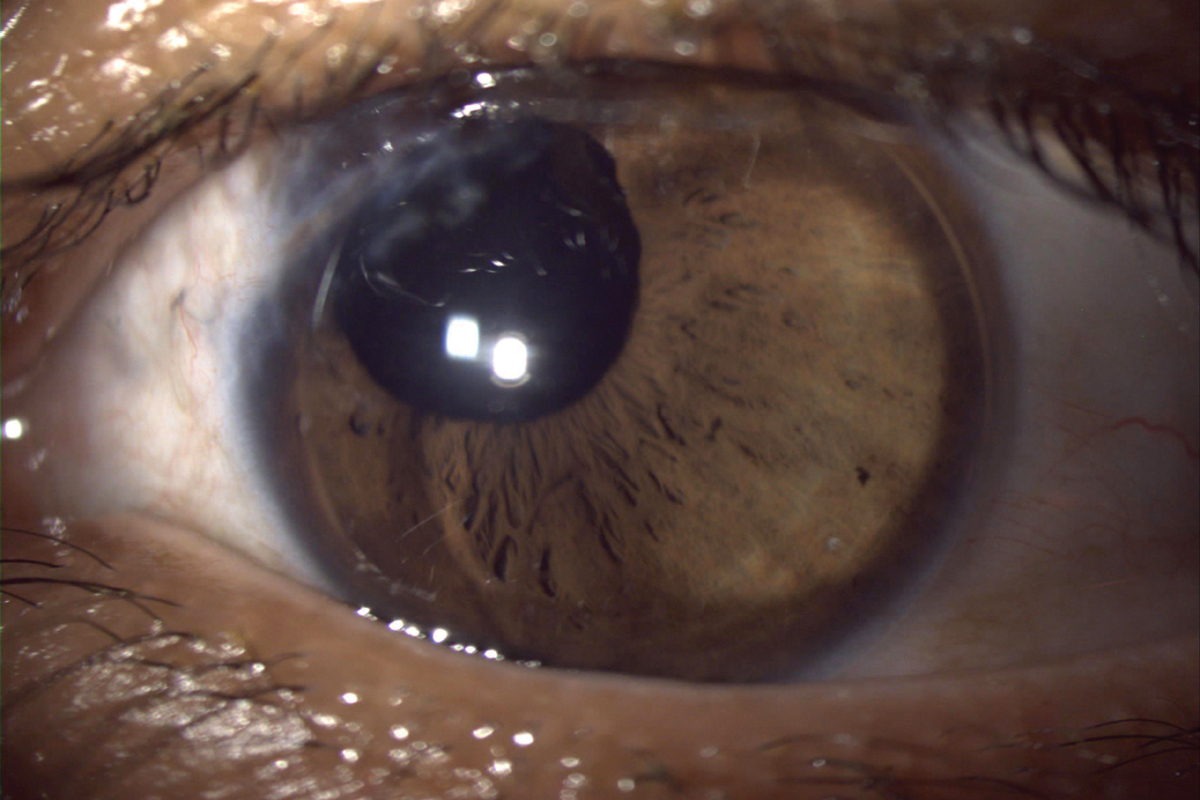
Fig. 3. Corneal lens on eye with nasal conjunctival sutures in Case #2. Centration and stability of the lens were important due to the nasally displaced pupil. Click image to enlarge. |
At the second dispensing visit, trace staining was present at the sutures. The larger diameter lens allowed for improved centration, and the patient noted better comfort and vision (Figure 3). At follow-up, the staining at the sutures had resolved and the lens was finalized. Polycarbonate spectacles with a reading prescription were recommended for protection.
While both patient cases presented their own fitting challenges, each were successful in corneal lenses. When fitting patients who have embedded sutures, it is crucial to follow up closely and ensure the sutures are unaffected by the contact lens wear. Consider altering the diameter to avoid any fitting obstacles or improve centration, and don’t forget to stress the importance of polycarbonate spectacles for protection!
The authors would like to acknowledge Bethany Peebles, executive director of consultation services at Art Optical, for her assistance with consultation in both of these cases.

